Health
When measuring heart attack risk, one important red flag is often overlooked, doctors say

Heart disease kills more people in the U.S. than any other cause of death — yet many Americans aren’t aware of one major genetic risk factor.
Lipoprotein(a), or Lp(a), is a protein that can greatly increase the chances of a heart attack when it’s present in high levels in the blood.
Fox News Digital spoke with Dr. Seth Baum, a cardiologist and chief scientific officer at Flourish Research in Boca Raton, Florida, about the importance of this often overlooked red flag.
COLORADO CARDIAC NURSE, AFTER THREE HEART ATTACKS, OFFERS SURVIVAL TIPS: ‘LISTEN TO YOUR GUT’
What is Lp(a)?
Along with low-density lipoprotein (LDL) and high-density lipoprotein (HDL), Lp(a) carries cholesterol through the blood.
The higher your levels of Lp(a), the more likely that cholesterol will build up in your blood vessels, increasing the risk of a heart attack or stroke.
Heart disease kills more people in the U.S. than any other cause of death — killing one person every 33 seconds. (iStock)
“Lp(A) contains a particle that leads to cardiovascular disease when it’s in higher concentrations,” Baum said.
There are three main elements of Lp(A) that put people at risk, the cardiologist said.
REDUCING SALT INTAKE BY JUST 1 TEASPOON A DAY HAS SAME EFFECT AS BLOOD PRESSURE MEDS, STUDY FINDS
The first is that it causes atherosclerosis, which is the buildup of fats and cholesterol in the arteries.
“Another is that it causes inflammation, which is a really important aspect of plaque progression and the risk of creating a heart attack,” Baum said.
The third component, which is also vital in the genesis of a heart attack or a stroke, is that Lp(a) increases the risk of clotting, the doctor said — which could block off the artery.
“We call it a triple threat,” Baum said.
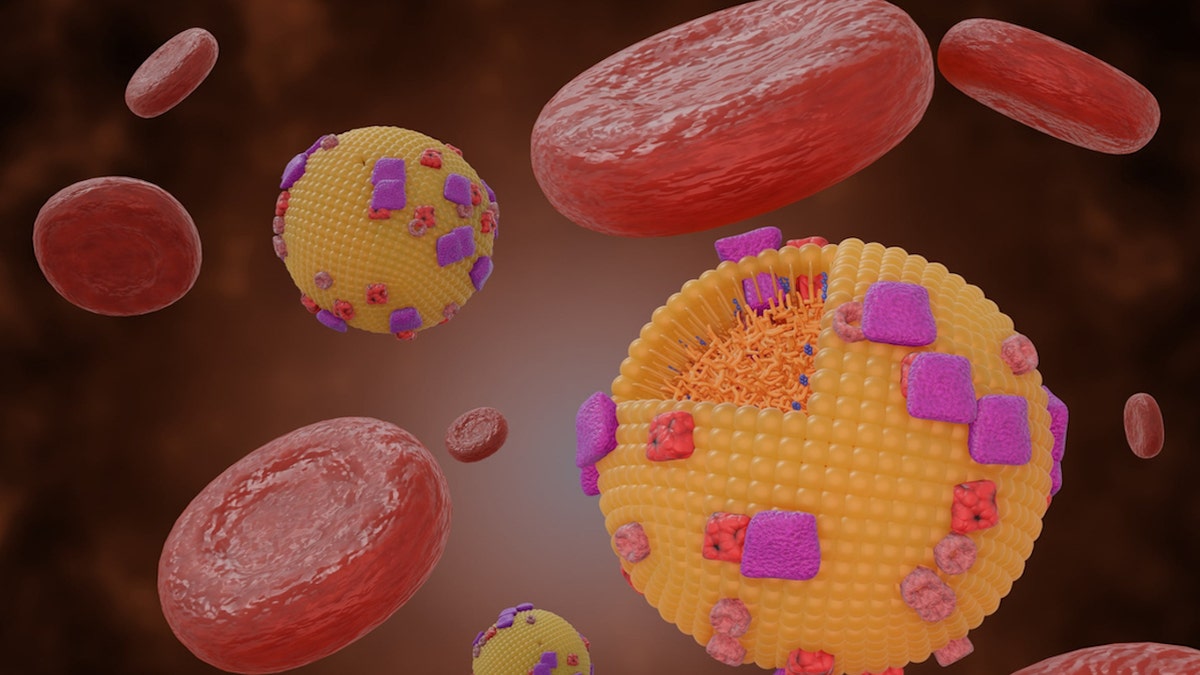
Along with low-density lipoprotein (LDL) and high-density lipoprotein (HDL), Lipoprotein(a) carries cholesterol through the blood. (iStock)
Brett Sealove, M.D., chief of cardiology at Jersey Shore University Medical Center, agreed that Lp(a) is an indicator of a serious threat.
“These ‘bad cholesterols’ result in plaque build-up in the arteries and reduced blood flow to vital organs, including the brain, heart, kidneys and legs,” he told Fox News Digital.
“The evidence is irrefutable — Lp(a) is considered an independent risk factor in addition to classic heart disease risk factors.”
Who is at risk?
Approximately 20% of the population is at risk because of Lp(a).
“These are very, very big numbers,” Baum said. “And it’s even higher than that in certain genetic groups.”
STANDING AND EVEN SLEEPING ARE BETTER FOR YOUR HEART THAN SITTING, NEW STUDY SUGGESTS
Black and South Asian Americans are at particularly high risk.
Despite that high prevalence, only a negligible share of Americans know their Lp(a) levels, the doctor pointed out.
“Probably fewer than 1% of the population has had their Lp(a) levels checked,” he estimated.

The higher your levels of Lp(a), the more likely that cholesterol will build up in your blood vessels, increasing the risk of a heart attack or stroke. (iStock)
Dr. Bradley Serwer, a cardiologist and chief medical officer at VitalSolution, a Cincinnati, Ohio-based company that offers cardiovascular and anesthesiology services to hospitals nationwide, noted that the cost and limited access to Lp(a) testing can be a problem.
“When trying to assess heart health risk, we often use risk screening tools that estimate an individual’s 10-year risk for developing significant cardiovascular disease,” he told Fox News Digital.
DOES THE FLU INCREASE THE RISK OF HEART ATTACKS?
“These calculators take into consideration age, gender, blood pressure, cholesterol levels and smoking history — but they do not include Lp(a),” he went on.
“Since these nationally accepted tools do not include the lipoprotein(a) in their score calculation, some insurance companies do not cover the cost of the testing.”
What can be done?
While LDL is genetically driven in a small subset of the population, Baum said, that type of lipoprotein is heavily influenced by diet and exercise.
Lp(A), however, cannot be controlled by lifestyle factors.
“There’s no therapeutic currently available that will reduce Lp(a),” Baum said.
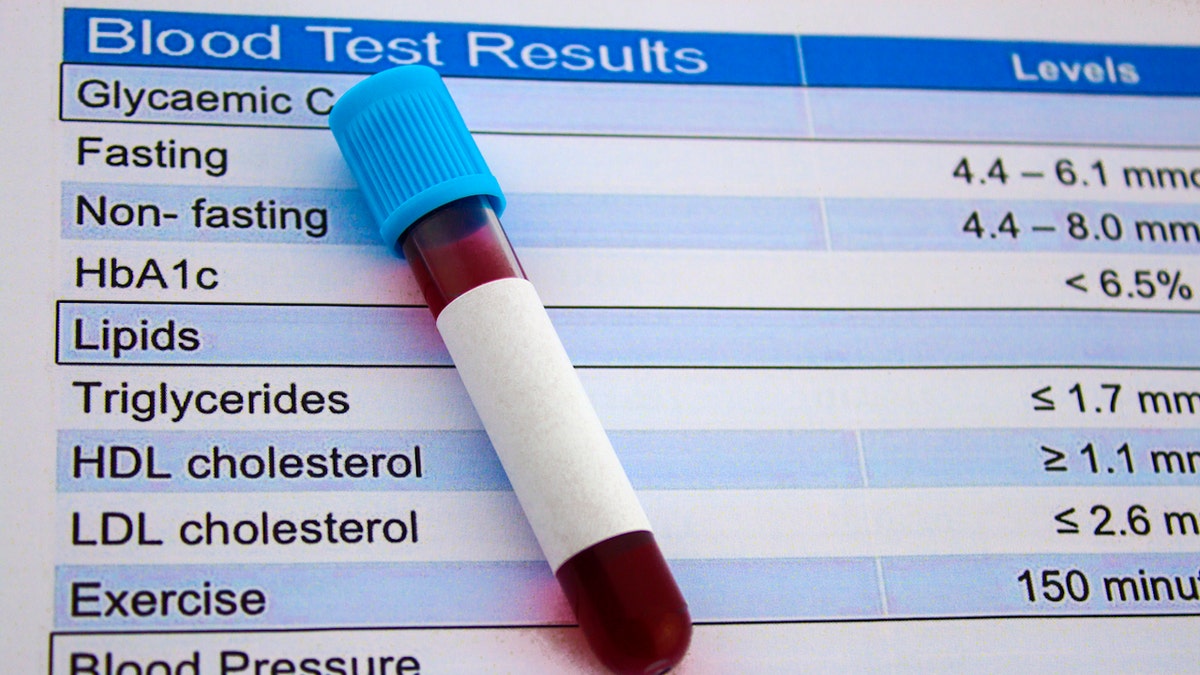
Lp(A) levels can be tested through a simple blood sample. (iStock)
So why check the levels if there’s nothing that can be done?
“Even though we can’t directly reduce Lp(a), we can reduce other cardiovascular risk factors,” Baum said. “You’ll still have the Lp(a) risk, but you won’t have all the other stuff floating around — so you can mitigate some of the overall risk.”
In Europe and Canada, the doctor noted, there are guidelines in place that state everyone should have universal screening for Lp(a) levels.
WANT TO LIVE LONGER? FOLLOW 8 HEART-HEALTHY HABITS, SAYS THE AMERICAN HEART ASSOCIATION
“In America, we’re a little behind the times — we still only check Lp(a) in patients who are at a higher risk,” he said.
Some doctors, like Baum, recommend testing Lp(a) levels for everyone, with the idea that if patients know they are more susceptible to heart attacks, they will be much more likely to reduce other cardiovascular risks.
Lp(A) levels can be tested through a simple blood sample.

At a minimum, Baum recommends getting Lp(a) levels checked at least once, and then again in the event of certain health changes. (iStock)
The levels tend to be relatively stable throughout the patient’s lifetime, the doctor said, but some elements can shift the Lp(a) a little in either direction.
“For example, going through menopause can dramatically increase Lp(a) levels, as can low thyroid or kidney disease,” Baum noted.
At a minimum, the doctor recommends getting Lp(a) levels checked at least once, and then again in the event of certain health changes.
“Probably fewer than 1% of the population has had their Lp(a) levels checked.”
Sealove agreed that patients should have their Lp(a) checked at least once as a screening test — “especially for those with a family history of heart disease and in conjunction with other laboratory parameters, including the standard lipid panel and other metabolic tests.”
In Serwer’s opinion, the decision of whether to test Lp(a) levels is a personal one that should be discussed with a medical provider.
“Before any medical test is ordered, it is important to know what you’re going to do with that information,” he told Fox News Digital.
Researchers are working to better understand Lp(a) and its role in diagnosis, risk assessment and potential therapeutics. (iStock)
“If knowing the Lp(a) level will make a difference or alter medical decisions, then it may be beneficial to measure.”
Regardless of the Lp(a) level, Serwer strongly recommends reducing cardiovascular risk factors with lifestyle, diet and exercise.
“The best way to combat atherosclerotic disease is to avoid it entirely — and the best way to do that is to start a healthy lifestyle as early as possible.”
Future of Lp(a) therapy
There is one therapy, called lipoprotein apheresis, that involves removing Lp(a) from the blood using IVs.
“It’s a technique we use to basically cleanse the blood of bad lipoprotein,” Baum said.
There are some drugs in development to treat high Lp(a).
Baum has a lipoprotein apheresis center in South Florida, and there are more than 40 other centers around the country.
This therapy is only available to a small number of patients, however.
CLICK HERE TO SIGN UP FOR OUR HEALTH NEWSLETTER
“We pretty much limit these for people who are very, very high risk,” Baum noted.
There are some drugs in development to treat high Lp(a), said Baum, who is heavily involved in clinical research.
“Those of us who know about these studies are very excited, because there is a real possibility that we’re going to do something significant in the not-too-distant future — that we’re going to have a therapeutic drug to reduce the risk of elevated Lp(a),” Baum said.

Regardless of the Lp(a) level, Serwer strongly recommends reducing cardiovascular risk factors with lifestyle, diet and exercise. (iStock)
Sealove reiterated that researchers are working to better understand Lp(a) and its role in diagnosis, risk assessment and potential therapeutics.
“Currently, several clinical trials are underway that target Lp(a), with more long-term outcome trials to come,” he told Fox News Digital.
“Until these treatments become available, patients and doctors should focus on optimizing traditional risk factors and educating themselves about the impact of Lp(a) on cardiovascular health.”
For more Health articles, visit www.foxnews.com/health.


Perhaps no vote was as agonizing for Senator Bill Cassidy, the Louisiana Republican and medical doctor, than his vote to confirm Robert F. Kennedy Jr. as President Trump’s health secretary. Mr. Cassidy wondered aloud for days how Mr. Kennedy, the nation’s most vocal and powerful critic of vaccinations, might handle an infectious disease crisis.
Now, as a measles outbreak rages in West Texas, Mr. Cassidy has found out. It all comes down, he said, to “the gestalt.”
On Monday, days after the Texas outbreak killed an unvaccinated child, Mr. Cassidy, the chairman of the Senate Health Committee, was clipping down a Capitol corridor when he was asked about Mr. Kennedy. He pointed to a Fox News Digital opinion piece in which Mr. Kennedy advised parents to consult their doctors about vaccination, while calling it a “personal” decision.
“That Fox editorial was very much encouraging people to get vaccinated,” he said.
Reminded that Mr. Kennedy had described it as a personal choice, Mr. Cassidy thought for a moment. “If you want to like, parse it down to the line, you can say, ‘Discuss with your doctor,’” Mr. Cassidy said. “He also said, ‘We’re making vaccinations available. We’re doing this for vaccination. We’re doing that for vaccination.’ So if you take the gestalt of it, the gestalt was, ‘Let’s get vaccinated!’”
Mr. Cassidy’s assessment — that the whole of Mr. Kennedy’s message was more than the sum of its parts — reflects how the measles outbreak has put a spotlight on how Mr. Trump’s unorthodox choice to run the country’s top health agency has brought a once-fringe perspective into the political mainstream, creating discomfort for some Republicans.
As the founder and chairman of his nonprofit, Children’s Health Defense, and later as a presidential candidate, Mr. Kennedy has repeatedly downplayed the benefits of vaccination. He has also repeatedly suggested that the measles, mumps and rubella vaccine causes autism, despite extensive research that has found no link.
Since winning Trump’s nod to head the sprawling Department of Health and Human Services, Mr. Kennedy has walked a careful line on the issue. Some of his recent statements, in which he stops short of denouncing vaccines, have angered some of his supporters. But his less than full-throated endorsement of vaccination, and his promotion of alternative remedies to treat measles, have angered mainstream scientists who say the one proven way to prevent measles is the vaccine.
“This, I would say, is the barest of the bare minimum that one can do in the middle of a measles outbreak,” said Dr. Adam Ratner, a New York City pediatrician who just published a book, “Booster Shots,” that warns of a measles resurgence.
But Del Bigtree, Mr. Kennedy’s former communications director and one of his closest allies, said Mr. Kennedy was doing exactly what he said he would do: putting all options on the table and letting parents decide for themselves.
He used the word “balance” to describe Mr. Kennedy’s approach, and said the media was being “incredibly disingenuous and in some ways alarmist and dangerous by creating a panic over a death from measles.”
Asked about Mr. Cassidy’s “gestalt” remark, Andrew Nixon, a spokesman for the department, referred back to the Fox opinion piece. He said the health secretary’s comment could speak for itself: “Vaccines not only protect individual children from measles, but also contribute to community immunity, protecting those who are unable to be vaccinated due to medical reasons.”
Mr. Cassidy, a liver specialist, made his career in medicine treating uninsured patients as a doctor in Louisiana’s charity hospital system. He is a fierce proponent of vaccines.
But he is also facing a Republican primary challenger in 2026, and voting against Mr. Kennedy risked prompting Mr. Trump to endorse his opponent — and sparking a potential backlash among an increasingly vaccine-skeptical G.O.P. electorate.
Mr. Kennedy’s “medical freedom” movement, which he calls “Make America Healthy Again,” is now deeply entrenched in the Republican Party. The coronavirus pandemic turned many conservatives against vaccine mandates, even for children attending school. Around the country, nearly 1,000 candidates, nearly all Republican, ran for elective office in November with the backing of Stand for Health Freedom, a Florida nonprofit that has pushed to make it easier for parents to opt out of school vaccine requirements.
For Mr. Cassidy and other Republicans who were uneasy about Mr. Kennedy, the situation in West Texas is forcing a reckoning, said Whit Ayres, a Republican strategist who is also a member of Rotary International, an organization that has set a goal of ending polio by promoting vaccination around the world.
“His position on vaccines was exceedingly well known when he was nominated, and when he was confirmed by the United States Senate,” Mr. Ayers said. “Everybody, with their eyes open, knew that his positions could lead to a resurgence of measles.”
As vaccination rates have dropped around the country, public health experts have warned that measles would be the first infectious disease to come back. But the Texas measles outbreak cannot be blamed on Mr. Kennedy. The disease began spreading within the Mennonite community, an insular Christian group that settled in West Texas in the 1970s; many Mennonites are unvaccinated and vulnerable to the virus.
Mr. Kennedy minimized the situation in Texas during a Cabinet meeting with Mr. Trump last week, saying measles outbreaks in the United States are “not unusual.” His Fox opinion piece promoted the use of vitamin A, which studies have shown is useful in treating measles in malnourished children.
He followed up with a prerecorded Fox News interview that aired on Tuesday, in which he said parents and doctors should consider alternative approaches, including cod liver oil, for the treatment of measles. He also acknowledged that vaccines “do prevent infection.” But once again, Mr. Kennedy did not urge Americans to get vaccinated.
The Texas Department of Health issued a health alert on Jan. 23 reporting two cases of measles. Since then, nearly 160 people have contracted the illness and 22 have been hospitalized. The Centers for Disease Control and Prevention said Tuesday that it had sent some of its “disease detectives” to Texas to support local officials in the response.
By Wednesday, while Mr. Cassidy appeared satisfied with Mr. Kennedy’s handling of the matter, the senator was pushing another key health nominee on questions of measles, vaccines and autism.
He wanted to know whether Dr. Jay Bhattacharya, appearing before the Senate health committee for his confirmation hearing as Trump’s pick to lead the National Institutes of Health, intended to spend tax dollars on research into the discredited theory that vaccines cause autism. Mr. Cassidy had repeatedly, and unsuccessfully, tried to get Mr. Kennedy to reject that theory in his own confirmation hearing.
Dr. Bhattacharya told the senator he was “convinced” that there is no link between the measles vaccine and autism. But like Mr. Kennedy, he said he supported additional research, if only to assuage the fears of nervous parents.
Mr. Cassidy was incensed, saying the matter had already been settled by years of extensive research. New studies, he said, would waste taxpayer dollars and take away money from studies that might uncover the true causes of autism. He pounded his fist on the table.
“If we’re pissing away money over here,” he said with a wave of his hand, “that’s less money that we have to actually go after the true reason.”
And in any event, Mr. Cassidy said, further research would not change minds. “There’s people who disagree that the world is round,” he said, adding, “People still think Elvis is alive.”
To secure Mr. Cassidy’s vote last month, Mr. Kennedy made a series of concessions, which Mr. Cassidy outlined in a Senate floor speech. They included a pledge not to disband the committee of experts that advises the Centers for Disease Control and Prevention on vaccines, and to leave intact statements on the C.D.C.’s website saying that vaccines do not cause autism.
Mr. Kennedy also promised to have an “unprecedentedly close collaborative working relationship” with Mr. Cassidy, and to meet or speak with him “multiple times a month,” and to give Congress advance notice of any vaccine policy changes.
“I will carefully watch for any effort to wrongfully sow public fear about vaccines between confusing references of coincidence and anecdote,” Mr. Cassidy said then.
On his way into the Senate chamber on Monday, he said he thought Mr. Kennedy was doing a good job with the Texas response. “He’s handling it well,” the senator said. He was asked if he had spoken to Mr. Kennedy about the measles outbreak.
“We speak on a regular basis,” Mr. Cassidy said, adding: “Let’s leave it at that.”

Obesity has long been classified as a global epidemic — and new data published in The Lancet journal spotlights how much worse it could get.
A team of researchers found that in 2021, one billion men and 1.11 billion women over 25 years of age worldwide qualified as overweight or obese — twice as many as in 1990.
In 2021, more than half of the world’s overweight and obese adults lived in eight countries: China (402 million), India (180 million), the U.S. (172 million), Brazil (88 million), Russia (71 million), Mexico (58 million), Indonesia (52 million), and Egypt (41 million), according to a press release.
THIS DISEASE KILLS MORE PEOPLE THAN ALL CANCERS AND ACCIDENTS COMBINED
If the increase continues at this same pace, the study projects that more than half (57.4%) of men and 60.3% of women will be overweight or obese by 2050.
In 2021, one billion men and 1.11 billion women over 25 years of age worldwide qualified as overweight or obese — twice as many as in 1990. (iStock)
The three countries expected to have the highest rates of overweight or obesity by 2050 are China (627 million people), India (450 million) and the U.S. (214 million).
The study also found that by 2050, nearly one-quarter of obese adults will be 65 or older.
The researchers analyzed data from the Global Burden of Diseases, Injuries, and Risk Factors Study, spanning 204 countries and territories.
OZEMPIC’S HEALTH BENEFITS KEEP GROWING, BUT ARE THE RISKS WORTH IT?
“The unprecedented global epidemic of overweight and obesity is a profound tragedy and a monumental societal failure,” said lead author Professor Emmanuela Gakidou from the Institute for Health Metrics and Evaluation (IHME), University of Washington, in the release.
“Governments and the public health community can use our country-specific estimates on the stage, timing and speed of current and forecasted transitions in weight to identify priority populations experiencing the greatest burdens of obesity who require immediate intervention and treatment, and those that remain predominantly overweight and should be primarily targeted with prevention strategies.”

The three countries expected to have the highest rates of overweight or obesity by 2050 are China (627 million people), India (450 million) and the U.S. (214 million). (iStock)
Another finding was that “more recent generations are gaining weight faster than previous ones and obesity is occurring earlier.”
This increases the risk of younger people developing obesity-related conditions like type 2 diabetes, high blood pressure, cardiovascular diseases and multiple cancers.
“The world has two choices: Act aggressively now or pay an unfathomable price later.”
There were some limitations to the study, the researchers acknowledged.
“Predictions are constrained by the quantity and quality of past data as well as systemic biases from self-reported data, which are likely to remain despite attempts to correct for bias,” they wrote.
They also noted that the definition of overweight and obesity is based on BMI (body mass index), “which does not account for variations in body structure across ethnic groups and subpopulations.”
The study also did not take into account the effects of GLP-1 anti-obesity medications and other interventions.

If cases rise to the study’s projections by 2050, a doctor warned that “obesity-related diseases will cripple healthcare systems worldwide.” (iStock)
Brett Osborn, a Florida neurosurgeon and longevity expert at Senolytix, called out obesity as the “single greatest modifiable threat to longevity, economic stability and national security.”
“Yet, instead of confronting the problem head-on, our culture continues to coddle bad habits, normalize obesity and abandon personal responsibility,” he said in a statement to Fox News Digital.
WEIGHT LOSS MAY BE HELPED BY DRINKING THIS, STUDY SUGGESTS
“This crisis is not about food deserts genetics or corporate greed — it’s about choices. And we are making the wrong ones.”
The obesity crisis can be linked to sedentary lifestyles, ultraprocessed foods and an “entitlement mentality that demands a pill for every problem,” according to Osborn.

The obesity crisis can be linked to sedentary lifestyles, ultraprocessed foods and an “entitlement mentality that demands a pill for every problem,” according to one doctor. (iStock)
“The reality is simple: Obesity is caused by caloric surplus and a lack of movement,” he said. “When you consistently eat more calories than you burn, you gain weight. Period.”
If cases rise to the study’s projections by 2050, Osborn warned that “obesity-related diseases will cripple healthcare systems worldwide.”
CLICK HERE TO SIGN UP FOR OUR HEALTH NEWSLETTER
“The recent Lancet study projects over 1.3 billion global diabetes cases and more than two million obesity-driven cancers annually,” he said. “Cardiovascular disease will double in prevalence across multiple regions, and the economic burden will exceed $4 trillion per year. This is unsustainable.”
“Our healthcare system was never designed to support a world where over half the population has a preventable, self-inflicted disease.”

“The time to fight obesity — relentlessly and unapologetically — is now.” (iStock)
The fight against obesity isn’t about aesthetics, Osborn said — “nor is this a personal affront to overweight or categorically obese people. This is about survival.”
“The world has two choices: Act aggressively now or pay an unfathomable price later,” he went on.
“The time to fight obesity — relentlessly and unapologetically — is now.”
For more Health articles, visit www.foxnews.com/health
The study was funded by the Bill & Melinda Gates Foundation. It was conducted by the GBD 2021 Adolescent and Adult BMI Collaborators. Fox News Digital reached out to the researchers for comment.

Therapy has been a part of Katerina Kelly’s weekly routine since elementary school, when a teacher suggested counseling for the 8-year-old.
At the time, Katerina’s autism was affecting their ability to manage time, make decisions and socialize. And for many years, the therapist seemed helpful. But once college rolled around, things changed.
“I always left counseling feeling either worse than I started — or numb,” said Mx. Kelly, 29, who lives in Natick, Mass, and uses they/them pronouns.
The skills that Mx. Kelly’s therapist had taught her in childhood weren’t translating as well now that she was older. In other words, they had hit a rut — the therapy, and the therapist, were not producing the desired results.
A therapy rut can feel disheartening, but it doesn’t have to end your pursuit of better mental health. We asked psychologists how to identify whether you’ve reached a sticking point and what to do about it.
What exactly is a therapy rut?
If you’ve hit a rut, you may feel as if your therapy sessions have stalled or become unhelpful, said Jameca Woody Cooper, president of the Missouri Psychological Association.
You may be emotionally disconnected from your therapist or less trusting of their plan. Perhaps you’re uncomfortable and tense during therapy, or you’ve started to dread or miss appointments, Dr. Woody Cooper added.
A rut can translate into “increased irritability while you’re in session, or a feeling of being misunderstood,” she said.
There are many reasons a rut can happen, the experts said:
-
You’ve made as much progress as you can in therapy at this time.
-
You would benefit from a different therapist or approach.
-
You need a new therapy goal.
-
You don’t need sessions as frequently as you did in the past.
-
Your expectations aren’t aligned with those of your therapist.
-
You’re not ready to explore past trauma or a difficult issue.
Mx. Kelly had experienced some of these roadblocks in her relationship with her childhood therapist.
“When I did try to bring up new things I was told we could work on it in the ‘next session,’ but that never came to be,” they said. “I hit a point where I started feeling so low.”
So Mx. Kelly began searching for a new therapist — it took more than six months, but they found someone who took their insurance and was a better fit.
If you’re feeling stuck, your therapist will ideally sense it too, said Regine Galanti, a therapist in Long Island who specializes in treating anxiety with exposure therapy.
“When I’m having the same conversations for more than two weeks in a row — that makes my warning bells start to go off,” she said.
That’s when it’s time to re-evaluate a client’s therapy goals, she added.
What can you do about a rut?
Don’t jump the gun by quitting therapy after one or two unproductive sessions, experts said.
“It’s unfortunately not uncommon to occasionally have a therapy session that feels like a dud,” said Alayna Park, an assistant professor of psychology at the University of Oregon.
But if after three or four sessions you feel like you haven’t learned any new coping skills or gained a better understanding of your problem, then it’s time to speak up, either during the session or in an email.
Dr. Park suggested a few ways to kick off the discussion: “I feel like my progress has stalled,” or “I would like to transition to learning new or different coping skills,” or simply: “I feel like I’m in a therapy rut.”
It’s also valuable to ask your therapist how many sessions you might need, what your progress ought to look like and how your therapist is measuring it, said Bethany A. Teachman, a professor of psychology and the director of clinical training at the University of Virginia.
Although it can make some people feel uneasy to voice their concerns, the experts said, a good therapist will not get angry or annoyed.
“Good therapy empowers patients” to do hard things, Dr. Teachman said.
How do you know if it’s time to take a break?
If you’ve talked with your therapist about your concerns and nothing has changed, you may want to consider taking a break.
Stepping away can offer “a sense of agency, and time to evaluate if the current therapeutic relationship is the correct one,” Dr. Woody Cooper said.
During this break, you can take time to think about your feelings and behavior, explore different types of therapy or try out another therapist, she added.
Annie Herzig, an author and illustrator who lives in Fort Collins, Colo., decided to take a step back after a few months of seeing a new therapist, when she hadn’t noticed any improvement in her mood.
Ms. Herzig, 43, finally sent her therapist an email saying she wasn’t getting what she needed from their sessions.
Taking time away was helpful — Ms. Herzig found a different therapist who she has now been seeing for four years.
“I feel energized at the end,” Ms. Herzig said of their sessions together. “Even if I cry my eyes out.”

Georgia Tech students help Savannah woman trace her lineage back 6 generations, despite the impacts of slavery

Beloved Hawaii Island teacher, wrestling coach retires after 44 years

Despite earlier concerns, governor signs largest income tax cut in Idaho history – East Idaho News

Game Preview | #18 Purdue at Illinois | Boilers set eyes on double bye

NCAA Tournament bubble watch: OSU-Indiana looms large, UNC faces win-and-in game

Why Marjorie Taylor Greene was ‘kicked out’ of the Freedom Caucus according to Rep. Buck

Colorado Rockies game no. 116 thread: Zac Gallen vs José Ureña

See it: Tesla crashes into Columbus convention center at 70 mph

Fox News Politics: Georgia the whole day through

Death of missing Oregon girl found in stream ruled homicide

Federal Workers Who Were Fired and Rehired by the Trump Administration

Trump FDA nominee turns vaccine question on Dem, recalling controversial Biden decision

Trump again spreads baseless claims about Trudeau, Canada’s election

Steve Carell announces that a charity will fund proms for students affected by LA fires

Who Paid for Trump’s Transition to Power? The Donors Are Still Unknown.
-
 Sports1 week ago
Sports1 week agoNHL trade board 7.0: The 4 Nations break is over, and things are about to get real
-
 News1 week ago
News1 week agoJustice Dept. Takes Broad View of Trump’s Jan. 6 Pardons
-
 World1 week ago
World1 week agoHamas says deal reached with Israel to release more than 600 Palestinians
-
 Science1 week ago
Science1 week agoKilling 166 million birds hasn’t helped poultry farmers stop H5N1. Is there a better way?
-
 News1 week ago
News1 week agoChristianity’s Decline in U.S. Appears to Have Halted, Major Study Shows
-
 World1 week ago
World1 week agoGermany's Merz ‘resolute and determined,' former EU chief Barroso says
-
 Technology1 week ago
Technology1 week agoMicrosoft makes Copilot Voice and Think Deeper free with unlimited use
-
 Politics1 week ago
Politics1 week agoSome Republicans Sharply Criticize Trump’s Embrace of Russia at the U.N.