Science
Mounjaro bests Ozempic for weight loss in first head-to-head comparison of real-world use

In the first head-to-head comparison of two blockbuster drugs used in real-world conditions, people who took Mounjaro lost significantly more weight than their counterparts who took Ozempic — and the longer the patients kept taking the drugs, the wider the gap became.
After three months of weekly injections, patients on Ozempic lost 3.6% of their body weight, on average, while those on Mounjaro lost an average of 5.9%.
At the six-month mark, Ozempic patients had dropped an average of 5.8% of their weight, while the average weight loss for Mounjaro patients was 10.1%.
And when a full year had passed, those taking Ozempic had lost an average of 8.3% of their weight, while those taking Mounjaro had shed an average of 15.3%.
The researchers who conducted the analysis also found that compared with people on Ozempic, those on Mounjaro were 2.5 times more likely to lose at least 10% of their initial weight and more than three times as likely to lose at least 15% of their weight during their first year on the medications.
The findings were published Monday in JAMA Internal Medicine.
Dr. Matthew Freeby, an endocrinologist and director of the Gonda Diabetes Center at UCLA’s Geffen School of Medicine, said the study results are in line with what he has observed in his own patients.
“From a weight-loss perspective, and from a sugar-lowering perspective for those with Type 2 diabetes, we see stronger effects with Mounjaro compared to Ozempic,” said Freeby, who was not involved in the research.
Both drugs were approved by the U.S. Food and Drug Administration to help people with diabetes keep their blood sugar under control. By mimicking a hormone called glucagon-like peptide 1, or GLP-1, they boost the body’s production of insulin, slow digestion, increase feelings of satiety and reduce appetite.
Mounjaro also imitates a related hormone called glucose-dependent insulinotropic peptide, or GIP.
When the drugs were tested against placebos in clinical trials, both helped patients lose a significant amount of weight. Tirzepatide, the active ingredient in Mounjaro, appeared to be more effective than semaglutide, the active ingredient in Ozempic. But the trials weren’t conducted under the same conditions, so the results aren’t directly comparable.
Researchers from Truveta, a healthcare data and analytics company owned by 30 health systems, sought to remedy that by examining their trove of electronic health records. The work also gave them a chance to see how patients fared outside the idealized setting of a clinical trial, which typically provides free medication, regular check-ups and other types of support.
With the help of their database, the researchers were able to spot people who filled their first prescription for either drug between May 2022 — the month Mounjaro joined Ozempic in receiving FDA approval — and September 2023. Patients didn’t need to have Type 2 diabetes to be included in the study, but they did have to be overweight (with a body mass index of at least 27) or obese (with a BMI of at least 30).
The Truveta team found about 41,000 people across more than 30 states who met all their criteria for being included in the study. Since Ozempic patients outnumbered Mounjaro patients by a margin of 3-to-1, the researchers used information on age, race, income, health history and other factors to come up with a group of Ozempic patients that most closely matched the Mounjaro patients. The result was a population of nearly 18,400 who were evenly split between the two drugs.
Before their first medication dose, the average weight for people in both groups was 243 pounds. But it didn’t take long for the two groups to diverge.
After accounting for unmeasured influences that could have skewed the results, the Truveta team found that the amount of weight lost was 2.4 percentage points higher for Mounjaro patients than for Ozempic patients after three months, 4.3 percentage points higher after six months, and 6.9 percentage points higher after a year.
Mounjaro also bested Ozempic in terms of people’s success in meting various milestones within a year of starting on one of the drugs.
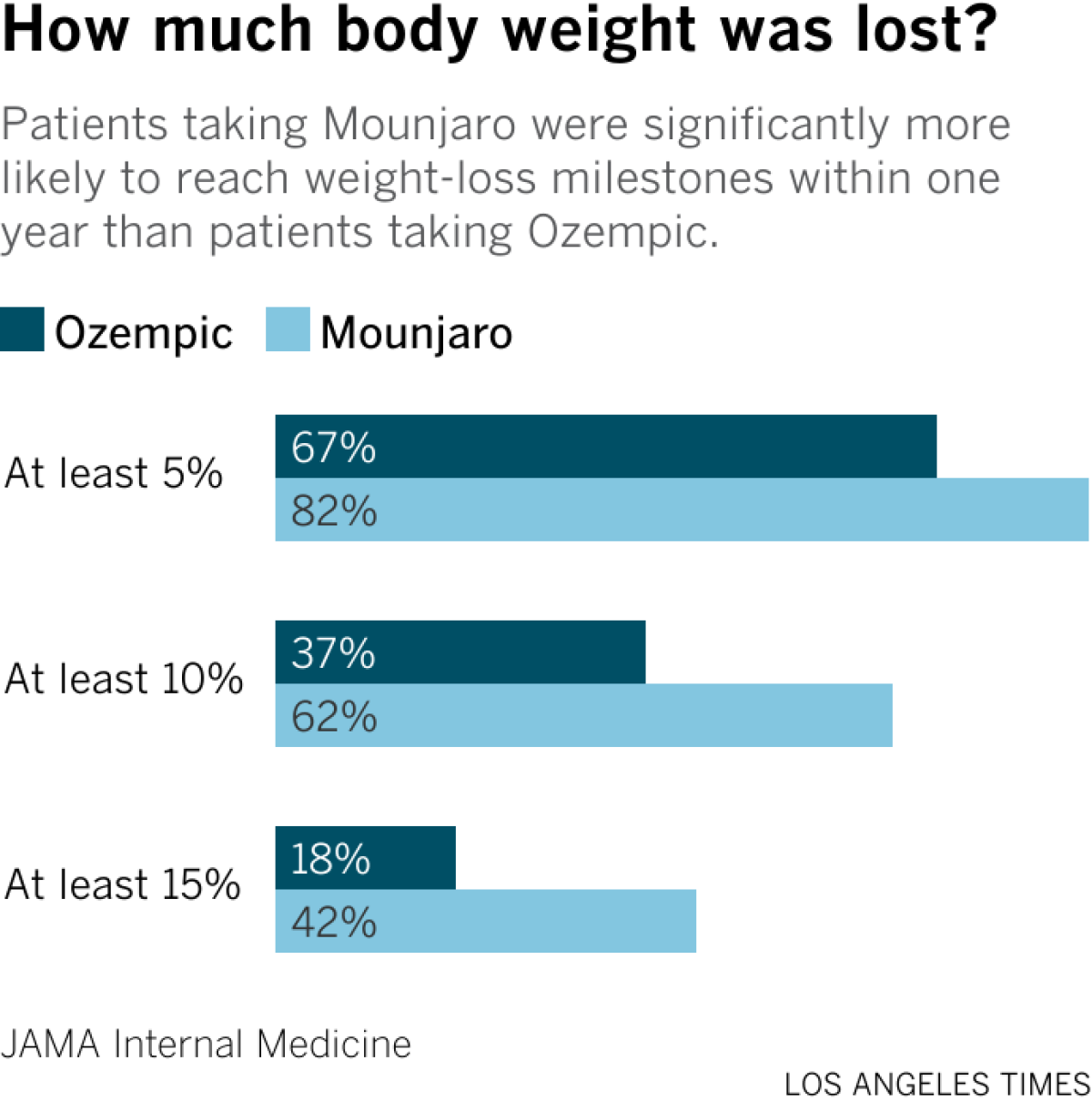
Nearly 82% of Mounjaro patients lost at least 5% of their body weight, compared with 67% of patients who took Ozempic. Likewise, 62% of Mounjaro patients and 37% of Ozempic patients lost at least 10% of their initial weight, while 42% of Mounjaro patients and 18% of Ozempic patients lost at least 15% of their starting weight.
The researchers didn’t examine the biological mechanisms of the two drugs, but study leader Tricia Rodriguez, a principal applied scientist with Truveta Research, said Mounjaro may have been more effective because it works two ways instead of just one.
The big gap in effectiveness wasn’t accompanied by a measurable difference in the rate of moderate or severe side effects like bowel obstructions and pancreatitis, which were rare for patients in both groups. The researchers didn’t compare the risk of milder problems like nausea and vomiting because people wouldn’t necessarily report them to their doctors, Rodriguez said.
Regardless of which drug they took, patients with Type 2 diabetes lost less weight than patients without the disease, the researchers found. That might be explained by the fact that certain diabetes treatments can cause weight gain, and that some patients eat more throughout the day to keep their blood sugar from getting too low, Freeby said.
It’s also possible that people who sought prescriptions for Ozempic or Mounjaro with the goal of slimming down were more motivated to keep taking the drug even if it was expensive or caused uncomfortable side effects, or that they were more likely to adopt other behaviors that promote weight loss, Rodriguez said.
Figuring this out is “a crucial topic for future research,” she said.
People currently taking Ozempic likely have a more pressing question on their minds: Should I switch to Mounjaro?
Dr. Nick Stucky, an infectious disease physician at Providence Portland Medical Center and the study’s senior author, said the results alone should not cause patients to stop taking a drug that is working for them. The risk of side effects, insurance coverage and drug availability are things to consider as well.
“While tirzepatide was significantly more effective than semaglutide, patients on both medications experienced substantial weight loss,” said Stucky, who is also Truveta’s vice president of research.
Freeby seconded that opinion.
“If someone is doing well with a medication, why rock the boat?” he said.
Freeby added that Ozempic (and its sister medication Wegovy, which is FDA-approved specifically for weight loss) has at least one advantage over Mounjaro (and Zepbound, its weight-loss counterpart): In clinical trials, Ozempic has been shown to reduce the risk of heart attacks, strokes and other cardiovascular problems as well as kidney failure.
“At this point, we don’t have a lot of data on Mounjaro when it comes to secondary outcomes,” he said.

While it may not be remembered as FIFA’s most controversial decision of the 2026 World Cup, the institution of mandatory cooling breaks in all matches has been met with boos and derision, with critics saying the pauses disrupt the game’s flow and offer little benefit in air-conditioned environments.
“They’re in a dome here! Temperature-controlled, climate-controlled — why are we having a break?” fumed one England fan to a radio reporter outside the England-Croatia match in Arlington, Texas, where field temperatures inside AT&T Stadium approached a comfortable 70 degrees Fahrenheit despite an outdoor heat and humidity index near 105 degrees.
But for Dr. Bert Mandelbaum, chief medical officer for U.S. men’s soccer and vice chair of Cedars-Sinai Medical Center’s orthopedic surgery department, the breaks set an important precedent for prioritizing athlete health in extreme heat, even at the highest levels of competition.
“I do think the cooling breaks are an important part of the game. I’m really excited and happy that we are employing those,” he said by phone Tuesday morning, hours after the U.S. team’s 4-1 knockout loss to Belgium.
“Difficult weather environments bring on dehydration and can create severe exhaustion, heat exhaustion, and those [conditions] have tremendous and dire consequences,” Mandelbaum said. “Talk radio could discuss it over and over again, but from our standpoint, the real messaging should be to our communities, our club players, that this is an important part of our game, and the cooling break is how we help manage it.”
Warming climate conditions are forcing changes to human behavior all around the globe, including on the pitch.
Extreme heat kills more people each year than all other forms of extreme weather combined. Elite athletes are not immune to its effects.
As temperatures during a game rise, the circulatory system diverts blood to the skin to lower core body temperatures at the same time that active muscles require oxygen-rich blood. This places extra strain on the heart, which pumps harder to keep up with demand. Sweating players lose electrolytes faster than they can consume them, leading to muscle cramps, fatigue and dizziness.
Virtually all aspects of the game degrade in the heat, Mandelbaum said. Players’ performance, recovery ability and decision making erode. Artificial turf becomes intolerably hot, and the soil in natural grass can harden until it’s like playing on concrete. Air molecules inside the ball expand, making it a harder and faster object. Even fans risk injury: 22 people were treated for heat-related illnesses at a FIFA Fan Festival in Houston last month.
Mandelbaum directs the FIFA Medical Center of Excellence at Cedars-Sinai and was part of the FIFA Medical Committee in 2014, when the first World Cup cooling break was called during a Netherlands-Mexico match in Fortaleza, Brazil.
At the time, the sport’s governing body recommended hydration breaks if temperatures surpassed 102.2 degrees.
This year’s World Cup, hosted across the U.S., Canada and Mexico, is the hottest played since the tournament began in 1930. It has coincided with a withering heat wave in the eastern U.S. With a heat index of nearly 104 degrees at kickoff, the July 4 match in Philadelphia between France and Paraguay is believed to be the second-hottest game in World Cup history, after a 105-degree match in 1994 between Ireland and Mexico in Orlando, according to meteorologist Brad Maushart.
FIFA announced in December that this year’s tournament would be the first in which all matches must pause once in each half for hydration and cooling, regardless of temperature conditions.
FIFA President Gianni Infantino said mandatory breaks equalize playing conditions in all matches. When they haven’t been loudly booing, many fans have noticed that teams often appear to spend as much time strategizing during the pauses as they do hydrating.
Given this, “if we were to use hydration breaks only in those matches where it was too hot and not in the other matches, we would give an advantage or a disadvantage to some of the coaches or some of the teams,” Infantino told Sports News Television.
Harry Brown, a postdoctoral research associate at the University of Sydney’s Heat and Health Research Centre, expressed frustration over the universal breaks in an op-ed in the journal Nature.
“Although it might seem fair to treat all games in the same way, this blanket approach risks undermining trust in heat-safety measures. If breaks are always used, regardless of risk, they stop being meaningful and start looking like routine stoppages,” Brown wrote.
Without active efforts to lower players’ core temperatures, pausing game play may not be enough to effectively stave off heat injury, he wrote. In his own research, Brown’s team compared the effects of passive breaks against breaks with active cooling measures on the health of players participating in 90-minute soccer games in 104-degree heat and 41% humidity.
When players cooled themselves with cold drinks and icy towels during short breaks and took longer halftimes, their core temperatures and cardiovascular strain lowered considerably more than they did after only passive breaks, Brown wrote.
Other physicians argued that even an under-utilized break was better for athletes than nothing at all.
“I would say that it’s better to err on the side of having cooling breaks rather than risk not having them,” said Dr. Miho J. Tanaka, an associate professor of orthopedic surgery at Harvard Medical School who also serves as a team physician for the Boston Red Sox and the New England Revolution.
“Ultimately, an individualized screening or monitoring process may be the safest approach, but we are still far from being able to precisely identify and intervene when an individual player may be at risk,” she said. “Until we are able to do so, having standardized breaks is a step in the right direction, as long as teams and players are informed when to escalate their level of concern and take action when more aggressive measures are truly needed.”
While a cooling break is rarely medically necessary inside a climate-controlled indoor stadium, Mandelbaum said it still sends a valuable message to players around the world: If hydration breaks are a part of the sport’s biggest event, they should be allowed at every other level of play.
“Not only is [the hydration break] a good thing, it’s a necessary thing,” Mandelbaum said. “This is the world’s game … we have to figure out how to help players at all levels and ages to have the ability to thermoregulate, hydrate, how to do it well.”

A trio of satellites set to launch early Tuesday will give wildland firefighters more time to respond and scientists more information about fire-prone regions across the globe.
The launch from Vandenberg Space Force Base is the first phase in a constellation called FireSat that will eventually cover the globe with 50 satellites collecting high-resolution imagery of fires and conditions on the ground every 20 minutes.
Earth Fire Alliance, the nonprofit group behind FireSat, got the project off the ground with $69 million in grants from the Bezos Earth Fund, Google and the Gordon and Betty Moore Foundation.
San José-based Muon Space built the satellites. Muon and the California Department of Forestry and Fire Protection are both FireSat partners.
The satellites use advanced thermal sensors to detect heat and can pick up signals from fires as small as a beach bonfire, as well as cooler fires that have been smoldering for days, according to Michael Falkowski, lead scientist at Earth Fire Alliance. That information will help fire officials, including the Los Angeles and Los Angeles County fire departments, understand whether blazes are growing, where they are headed and how much soot and smoke they are generating.
FireSat’s infrared instruments detected this small roadside fire in Medford, Ore., during a 2025 test flight.
(Muon Space)
“If we can differentiate between a smoldering fire and a flaming combustion fire, it really has a big impact on how we can understand the air quality emissions coming off the fire,” Falkowski said.
Fires that burn at low temperature produce more harmful gases than hot fires. Think about a campfire. When it’s burning hot with bright flames, there is relatively little smoke. When it’s smoldering, it produces lots of thick, white or gray smoke.
Wildfires work the same way.
A hot, fast-burning fire has enough oxygen and heat to burn with more complete combustion, producing less smoke for every pound of wood burned.
Earth Fire Alliance will provide data from these first three satellites in the next few months to Cal Fire and fire agencies in Oregon, Texas, Australia and Portugal. Cal Fire will share it with Southern California fire agencies.
The network will also turn its sensors on in the Amazon Basin for the Brazilian nonprofit Amazon Environmental Research Institute.
Cal Fire should begin receiving data from the scientists later this year, according to Falkowski, who joined Earth Fire Alliance last year from NASA, where he was an earth science program manager running the agency’s fire science program.

Instruments on the satellites will be able to detect fires the size of a shipping container, and distinguish between hot, intense wildfires and cooler, smoldering ones.
(Muon Space)
Falkowski said the new FireSat satellites are a big improvement over existing ones because they will be able to see smaller fires with better resolution and distinguish low-intensity “cool” fires from high-intensity hot ones.
“The satellites are really designed to measure fire across the entire temperature profile, so we can see cool fires all the way up to really hot fires,” he said.
That kind of granular information is important for emergency responders in the field and planners who make decisions about calling for extra help or ordering evacuations.
The National Oceanic and Atmospheric Administration operates three satellites that can detect a fire somewhere inside a square 1,230 feet across.
In contrast, instruments on the FireSat satellites will be able to detect small brush and roadside fires 16 feet across.
Cal Fire officials have long embraced new technology to get ahead of wildfires in recent years, testing autonomous firefighting helicopters and partnering with UC San Diego to use artificial intelligence to filter images from a network of more than 1,200 cameras on lookout towers and mountain tops. The Alert California program is able to spot smoke in a video and sends automated messages to one of 21 agency command centers across California.
In 2025, Alert California sent out automated warnings before authorities even received 911 calls from the public 51% of the time, according to Phillip SeLegue, staff chief of Cal Fire’s intelligence program.

A worker at Mountain View-based Muon Space puts the final touches on a wildfire-detection satellite scheduled to launch Tuesday on a SpaceX rocket. The satellites will be tracking fires across the globe.
(Muon Space)
FireSat will help incident commanders get better information more quickly, and, unlike fire-spotting aircraft, the satellites can linger over a fire for days or weeks and aren’t hampered by high winds or smoke.
Travis Medema, chief deputy for the Oregon State Fire Marshall, said his office will use FireSat to plan escape routes and monitor fires. “If we can fight these when they are small, we feel we will be more efficient and can protect Oregonians,” he said.
One expert noted that turning satellite data into information useful to firefighters and forestry managers will take some time. The FireSat data will “be amazing for fire nerds, but how and whether it helps individual fires remains to be seen,” said Joe H. Scott, founder of Pyrologix, a wildfire analysis firm based in Missoula, Mont. “Right now, we are not basing decisions on where satellites tell us a fire is,” Scott said.
Pyrologix develops wildfire risk management models for federal agencies, local governments and utilities. Scott said FireSat’s high-resolution data will help him build better prediction models that take into account weather, drought, plants and the history of fires in a region.

California voters will decide 14 statewide propositions in the Nov. 3 election, measures placed on the ballot mostly by either powerful interest groups or lawmakers that will affect the lives of millions of Californians.
While a proposed tax on state billionaires has dominated headlines, voters will also have a chance to weigh in on a number of consequential issues, from healthcare to voter identification requirements and more.
Californians are accustomed to legislating by the ballot and often face a list of propositions. But even by the standards of the state’s direct democracy process, the 2026 election stands out. The campaigns supporting and opposing the ballot measures have already collected more than $100 million in contributions, and are expected to use their money to inundate the television airwaves, livestreams and social media feeds and to flood mailboxes with glossy campaign mailers over the coming months.
Here are the measures on the Nov. 3 ballot:
Proposition 1: The Veterans and Affordable Housing Bond Act of 2026
Spurred by the state’s affordable housing shortage, state lawmakers are asking voters to approve an $11.25-billion bond to boost affordable housing construction around the state.
Advocates say the funds would help build more than 40,000 shovel-ready affordable homes that are unable to move forward because of a financing gap and help preserve thousands of other existing units.
Proposition 1 includes specific funding for high-need groups, including $1.25 billion for a veterans’ home loan program, $1.15 billion for supportive housing for homeless people, $350 million for student housing at state universities, $450 million for farmworker housing and $200 million for Native American tribes.
“In California, we don’t turn away from the needs of our people — we meet them head-on,” said Gov. Gavin Newsom in a statement about the measure. “We are giving voters the power to help shape the future of housing in our state. This bond is about building communities, expanding access and affordability in California, where every family has a fair shot at a place to call home.”
Some Republicans took issue with the measure’s title — “The Veterans and Affordable Housing Bond Act of 2026” — arguing that it included veterans to have broader appeal while doing little to actually help homeless veterans.
“It’s a sad thing to say that you have to use the veterans as bait to get the people of the state of California to approve an $11-billion bond, and I just think that’s shameful,” said Sen. Shannon Grove (R-Bakersfield), an Army veteran. “Call it what it is. It’s a homeless bond, and it does include some veterans’ benefits, but it is not a veterans bond.”
Proposition 2: Save for California’s Future Act

This measure would give California lawmakers more flexibility over state spending and allow them to save money that could otherwise go back to taxpayers.
The measure, supported by Newsom, seeks to exempt deposits into state savings accounts from a spending limit that voters adopted through a series of ballot measures dating back to the late 1970s, and to increase the share of tax revenue that can be put into the rainy day fund.
Under an existing state appropriations restraint, also known as the Gann Limit, lawmakers cannot spend more than an amount determined by a formula that takes annual tax proceeds, changes to the population and cost of living into consideration. Tax revenue above the limit must be divided between schools and refunds to taxpayers.
The measure could incentivize lawmakers to save more money because funds tucked away in the rainy day fund would no longer be considered expenditures counted toward the spending limit. By allowing lawmakers to set aside more money that is not subjected to state spending limits, it could also allow them to hold onto money that otherwise would be returned to taxpayers under current law.
This proposed constitutional amendment was placed on the ballot by state lawmakers.
Proposition 3: Fund schools and healthcare

If passed, this proposition would make permanent an existing tax on high-income Californians.
The existing tax, passed by voters in 2012 and extended in 2016, is set to expire in 2031. It applies to people who earn more than $360,000 for single filers, $721,000 for joint filers, and $490,000 for heads of household. It adds between 1% to 3% to these high earners’ personal income tax rates.
According to the initiative text, the funds are largely earmarked for local school districts and community colleges, with some portion of the money going to California’s rainy day reserves — which the state uses to prevent cuts to healthcare and other services when revenues decline. The measure says revenues cannot be spent on state bureaucracy or administrative costs.
The state’s nonpartisan Legislative Analyst’s Office expects the measure to bring in between $5 billion and $15 billion annually, depending on how the stock market is performing, with the amount expected to grow over time.
Proposition 4: Public financing of campaigns

This measure would allow the state and local governments to offer public campaign financing to candidates running for elected office. Candidates receiving the funding must abide by expenditure limits and adhere to the criteria set by statute, ordinance or charter to demonstrate broad support, such as demonstrate a large number of small dollar contributions.
None of the public campaign financing can come from funds designated for education, transportation or public safety. The financing cannot discriminate based on party or whether a candidate is a challenger or an incumbent. The public funds cannot be used for legal costs, fines or to pay back personal loans to a campaign.
This measure was placed on the ballot by the California Legislature and governor.
Proposition 5: Recall elections
This measure would change the way recall elections are conducted in California. Under this proposed constitutional amendment, during a recall election, voters would decide solely whether a politician should be removed from their elected position. If the recall is successful, that office would remain vacant until it is filled in accordance with existing law — either by a separate election or by appointment.
Under current law, voters make two separate decisions during a recall election: Whether to remove the subject of the recall from office and, if they are booted, which candidate running to replace them should fill the position. The candidate who receives the most votes wins, even if they receive far less than 50% of the vote.
The proposed constitutional amendment would also allow the recalled politician to run in the next election to fill the vacancy, though they cannot be appointed to their former post. Under the current system, office holders targeted in a recall are barred from being a candidate to replace themselves in that same election.
The proposal comes in the wake of the unsuccessful, Republican-led recall campaign against Gov. Gavin Newsom in 2021, which in part tested voter sentiment about his response to the COVID-19 pandemic. One of the sponsors of the recall-reform measure was Sen. Josh Newman (D-Fullerton), who was recalled from office in 2018 after he voted to increase gas taxes for road repairs, legislation pushed by then-Gov. Jerry Brown. Newman won back his seat in 2020.
This proposed constitutional amendment was placed on the ballot by the California Legislature.
Proposition 37: Homeownership loan program

Proposition 37 would create a down payment assistance program to help middle-class Californians buy a new home.
The measure, spearheaded by former state Senate Majority Leader Bob Hertzberg, would allow middle-class California residents — defined as anyone who makes less than 200% of an area’s median income — borrow most of their down payment for a new home that they plan to live in. It is designed to boost construction of single-family homes.
A down payment is traditionally about 20% of the purchase price of a home. If passed, the measure would create a state-administered loan program that offers qualified homebuyers a second mortgage of up to 17% of a home’s sale price.
The proposition would allow the California Housing Finance Agency to issue up to $25 billion in revenue bonds to administer the program.
The Legislative Analyst’s Office does not anticipate the measure to result in direct state or local costs because the costs are meant to be covered by homeowners’ mortgage payments.
Proposition 38: Immunology research bond

Proposition 38 asks voters to approve an $8.4-billion bond to support research in the burgeoning fields of immunology and immunotherapy, which study the human immune system and how it can be used to prevent, treat and cure diseases.
If approved, half of the funding would go toward the creation of a new immunology and immunotherapy research institute affiliated with the University of California. The other half would fund research grants for other California-based universities and nonprofit medical research institutions to study potential treatments for cancer, Alzheimer’s disease and heart disease.
The measure has a built-in discount program for Californians — it requires that any technology or drugs developed from bond-funded research be sold to California patients for a price at least 20% below the national average.
Backers of the proposal include the Alzheimer’s Assn., National Multiple Sclerosis Society and other healthcare groups. Supporters argue the funding would facilitate research that could save lives and save patients “billions of dollars in health care costs by preventing and curing a range of debilitating diseases and illnesses,” according to the initiative text.
Proposition 39: Voter identification

Proposition 39 would require Californians to show government-issued identification every time they vote at the polls.
Currently, Californians must affirm under penalty of perjury that they are U.S. citizens and provide information to verify their identity, such as their birth date, driver’s license or Social Security number, when registering to vote, but they don’t have to present identification when they cast their ballot.
Under this measure, voters would also need to present government-issued ID each time they vote in-person at the polls or, if voting by mail, provide the last four digits of a “unique identifying number from government-issued identification” that matches the one they provided when they registered to vote. California would be required to provide free voter ID cards on request, and state and county election officials would be required to verify registered voters are U.S. citizens by using government data.
The voter ID measure has support from Assemblymember Carl DeMaio (R-San Diego), who has framed it as necessary to prevent voter fraud and restore trust. It comes as President Trump is pushing for stricter voter identification requirements and severe limits on voting by mail.
Democrats and voting rights groups, including the American Civil Liberties Union, oppose the measure, saying California’s elections are already secure — voter impersonation and noncitizen voting cases are rare — and that it would make voting harder for many eligible voters, including people who have changed names, move frequently or face housing instability.
According to the Legislative Analyst’s Office, the measure would make election administration more expensive, costing state and local governments anywhere from tens of millions to low hundreds of millions of dollars annually, plus tens of millions in upfront implementation costs.
Proposition 40: Billionaire tax

This proposition, supported by a healthcare worker union, would impose a one-time tax of 5% on taxpayers and trusts with assets valued at more than $1 billion.
According to a state-prepared summary of the measure, 90% of the tax revenues would be spent on healthcare and 10% would fund food assistance or education-related programs. California’s richest residents would be able to spread the payments over five years.
The Legislative Analyst’s Office estimates it would generate “tens of billions of dollars” spread over several years, but would lead to an annual decrease in state income tax revenues of “hundreds of millions of dollars or more.”
Newsom has publicly opposed the tax, arguing it would lead wealthy residents to leave the state and lead to future budget problems. Other opponents include Planned Parenthood, the California School Boards Assn. and a nonprofit called Building a Better California that is backed by tech execs and venture capitalists.
Some billionaires have already proactively moved themselves or their businesses out of the state because of the proposal, which as written would retroactively apply to residents of the state as of Jan. 1.
Proposition 41: Requires limits and audits on new state special taxes

This is one of two ballot measures crafted by opponents of the proposed initiative to impose a new tax on California billionaires, and it would in effect undercut or curtail that wealth tax.
This proposed ballot measure would also prohibit any new state taxes from being excluded from the state’s current voter-approved spending limit. The proposed billionaire tax would have such an exclusion. If the billionaire tax proposal is approved by voters but this proposal receives more votes, the billionaire tax measure would be voided.
The measure would require the state auditor to conduct a financial and performance audit of proposed ballot initiatives and of the programs they fund. The measure would require audits of any program that would receive funding from the special tax in the proposed initiative to assess the efficiency of the program and recommend who ought to reduce its annual costs by 10%. If the measure passes, the costs of the audits would be paid via the revenues generated by the special tax.
This ballot initiative is one of two so-called poison pills to sink the billionaire tax that is being bankrolled by Building a Better California, which has raised well over $100 million from the state’s most affluent. The largest donor is Sergey Brin, a co-founder of Google, who has reportedly moved out of California because of the tax proposal. He donated at least $82 million to the group as of late June.
Proposition 42: Ban on new state personal property taxes
This is one of two ballot measures created by opponents of the proposed initiative to impose a tax on California billionaires, and it would in effect void that wealth tax.
This proposed ballot measure would prohibit new taxes on personal property, intellectual property, retirement accounts and other assets and would limit situations in which a ballot measure or state lawmakers can impose or raise taxes retroactively — both of which are essential parts of the billionaire tax initiative.
If the billionaire tax proposal is approved by voters but this proposal receives more votes, the billionaire tax ballot measure would be voided.
This ballot initiative is one of two so-called poison pills to sink the billionaire tax that is being bankrolled by Building a Better California, which has raised well over $100 million from the state’s most affluent. The largest donor is Sergey Brin, a co-founder of Google, who has reportedly moved out of California because of the tax proposal. He donated at least $82 million to the group as of late June.
Proposition 43: Voting thresholds for special taxes

The measure would prohibit local governments from imposing new special taxes unless the proposed tax receives approval from two-thirds of voters. The restriction also applies to citizen initiatives, which currently only need a simple majority vote to be approved.
The Howard Jarvis Taxpayers Assn. supports Proposition 43. The advocacy group has characterized the measure as an effort to “save” 1978’s Proposition 13, the landmark initiative that capped California property tax increases and required a super-majority of votes to approve most future tax increases.
Assemblymember Buffy Wicks (D-Oakland), who authored the legislation that became Proposition 43 — ACA 22 — opposes the measure and has urged Californians to vote against it. She said the only reason she crafted the bill was because it was a necessary bargaining chip to torpedo another ballot measure backed by the Howard Jarvis Taxpayers Assn. that would have devastated revenues for local governments and retroactively rescinded some local tax increases.
“I authored ACA 22 not because I wanted it to become law — but because it was the only path left to get the more dangerous initiative off the ballot before time ran out,” Wicks posted on social media.
Proposition 44: Regulate health clinic spending

If passed, Proposition 44 would require federally qualified health centers to spend 90% of their revenue on “program services advancing their charitable purpose” rather than management and overhead. Community clinics that fail to comply would be penalized, with fines placed in a state-managed fund to be spent on clinic workforce programs.
Advocates say clinics spend too much on executive pay and other administrative costs and not enough on patient care. The measure, which would dictate how clinics spend money, is designed to fix that. The measure is backed by the Service Employees International Union-United Healthcare Workers West, an influential healthcare workers union, which argues it will help hold clinics accountable.
In May, the California Primary Care Assn., which represents more than 2,300 community health clinics, sued to block the ballot measure. The state’s powerful doctors’ lobby, the California Medical Assn., also opposes the measure, arguing it would ban clinics from keeping funding in reserves and hamper their ability to upgrade equipment or expand to new locations.
The Legislative Analyst’s Office estimates that enforcing the measure would cost the government up to the low tens of millions annually, and that much of the cost would be paid for through penalties and fees charged to affected clinics. The office says the measure has “uncertain” impacts and could lead to clinic closures.
Proposition 45: CEQA reform
This proposition would amend the California Environmental Quality Act, or CEQA, and speed up the process for projects deemed “essential,” including certain housing, water, health, public safety, energy and transportation projects.
Jails, detention facilities and oil or natural gas production facilities would not be considered “essential” projects, according to the measure text.
If passed, the measure would set deadlines for public agencies to complete environmental review, allow expedited review of a project’s environmental impacts — currently, public agencies are required to consider a range of feasible alternatives to reduce environmental impacts — and establish deadlines for filing and resolving lawsuits.
CEQA lawsuits have often been used to block construction of housing in the state. For instance, in Berkeley, neighbors used CEQA — citing potential noise impact from partying students — to delay, for years, UC Berkeley’s construction of student dorms on People’s Park.
The Legislative Analyst’s Office estimates that the state and local government implementation will cost in the tens of millions of dollars for the first several years. It notes the legislation would probably result in net savings in the long term due to reduced administrative and legal workload.
Times staff writers Seema Mehta and Phil Willon contributed to this report.
-
 Politics6 minutes ago
Politics6 minutes agoPlatner’s collapsing campaign in Maine adds new midterm pressures for Democrats nationwide
-
Science8 minutes ago
Fans slam FIFA’s cooling breaks. Why the U.S. World Cup team doctor disagrees
-
 Sports14 minutes ago
Sports14 minutes agoCowboys’ Marshawn Kneeland had early-stage CTE when he died by suicide
-

 World24 minutes ago
World24 minutes agoRussian missiles strike Ukraine’s capital, Kyiv, for third time in a week
-
 News51 minutes ago
News51 minutes agoReigning champion Argentina escapes with remarkable World Cup victory over Egypt
-

 Los Angeles, Ca2 hours ago
Los Angeles, Ca2 hours agoPunk legends unite for special Ramones tribute in Los Angeles
-

 Detroit, MI2 hours ago
Detroit, MI2 hours agoFirefighters battle large blaze at vacant apartment complex on Detroit’s west side
-
San Francisco, CA3 hours ago
49ers Sign DL Gracen Halton to a Four-Year Deal



