Science
Deadly overdoses stopped surging among L.A. County homeless people. Narcan could be why

Year after year, Los Angeles County has seen devastating losses on its streets, as homeless people bedding down in tents, under tarps and on sidewalks have lost their lives to drug overdoses at soaring rates.
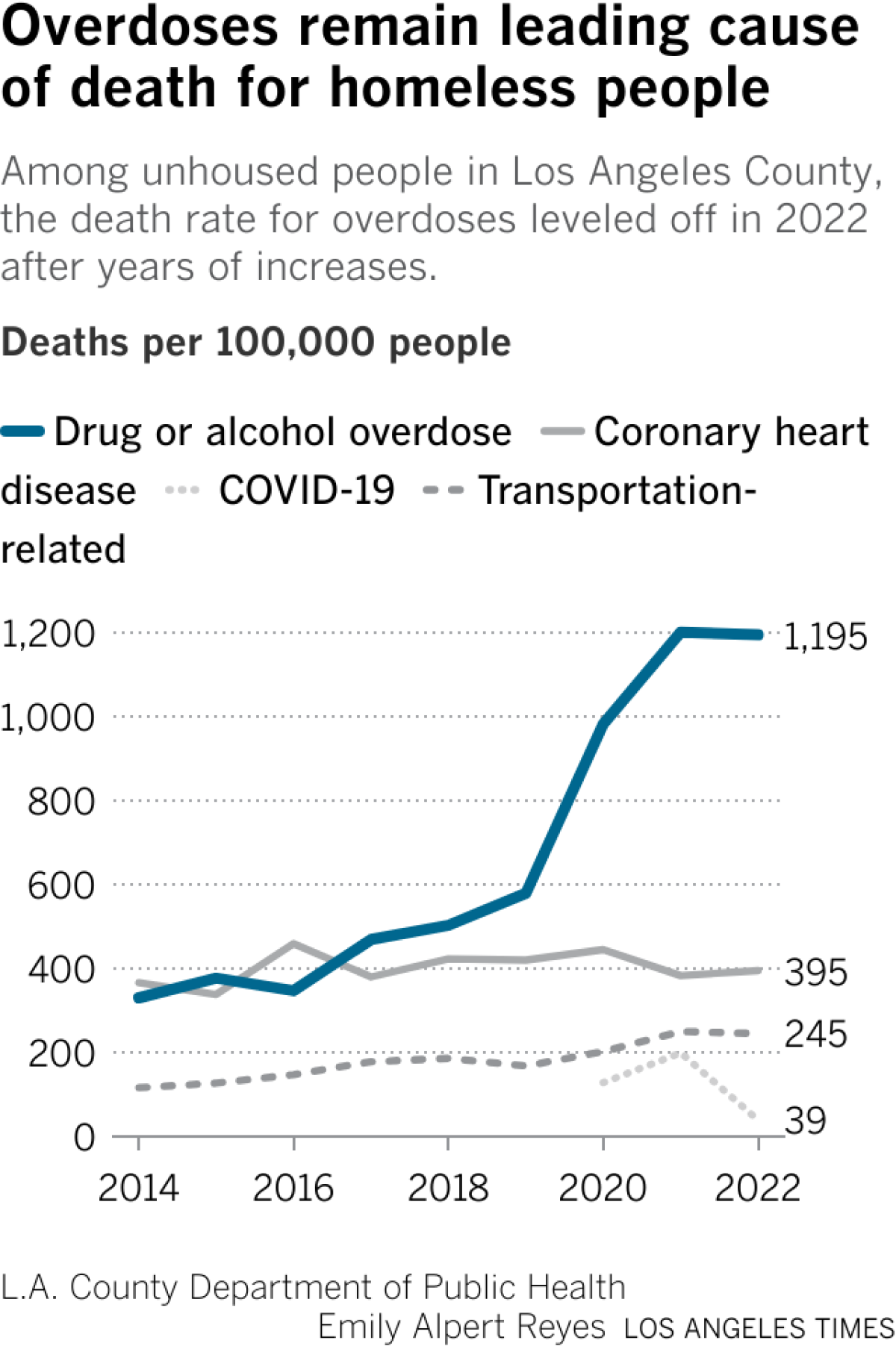
Now a newly released report shows the death rate from overdoses stopped rising among unhoused people in the county in 2022 — the same year L.A. County was stepping up its efforts to save lives.
Public health officials welcomed the news as a glint of hope, but cautioned it is too soon to say if the numbers are headed for a lasting downturn. They pointed to a county push to dramatically ramp up the distribution of naloxone — a medicine that bystanders can use to stop opioid overdoses — as a likely factor.
In their report, county officials touted a “near doubling” that year in the reported number of overdoses that were thwarted with naloxone, based on figures provided by a county program. The lifesaving medicine is commonly sold as a nasal spray under the brand name Narcan.
Two years ago in North Hollywood, Manny Placeres told The Times he had revived people seven times using Narcan that had been provided to him by a county team, honing his technique with time.
“As they’re knocking on heaven’s door, I pull them back,” Placeres said.
Manny Placeres, who has administered naloxone many times to reverse opioid overdoses on the streets, embraces Leimer in 2022.
(Christina House / Los Angeles Times)
The L.A. County Department of Health Services has handed out Narcan at homeless encampments, given it to community groups and county agencies and set up vending machines to dispense it for free to people leaving county jails.
As of February, the health services department said it had distributed more than 600,000 doses of naloxone since launching its initiative, resulting in more than 25,000 overdoses being stopped. Community groups and syringe programs have bolstered such efforts by handing out their own supplies of free naloxone provided by the state.
Dr. Gary Tsai, director of the public health department’s substance abuse prevention and control bureau, said that after years of alarming increases, “it is encouraging to see a slowing of this leading cause of death for people experiencing homelessness.”
“Efforts to increase access to naloxone and overdose prevention services have undoubtedly helped to bend this curve and provide a blueprint for reducing drug-related fatalities in this very high-risk population,” he said in a statement.
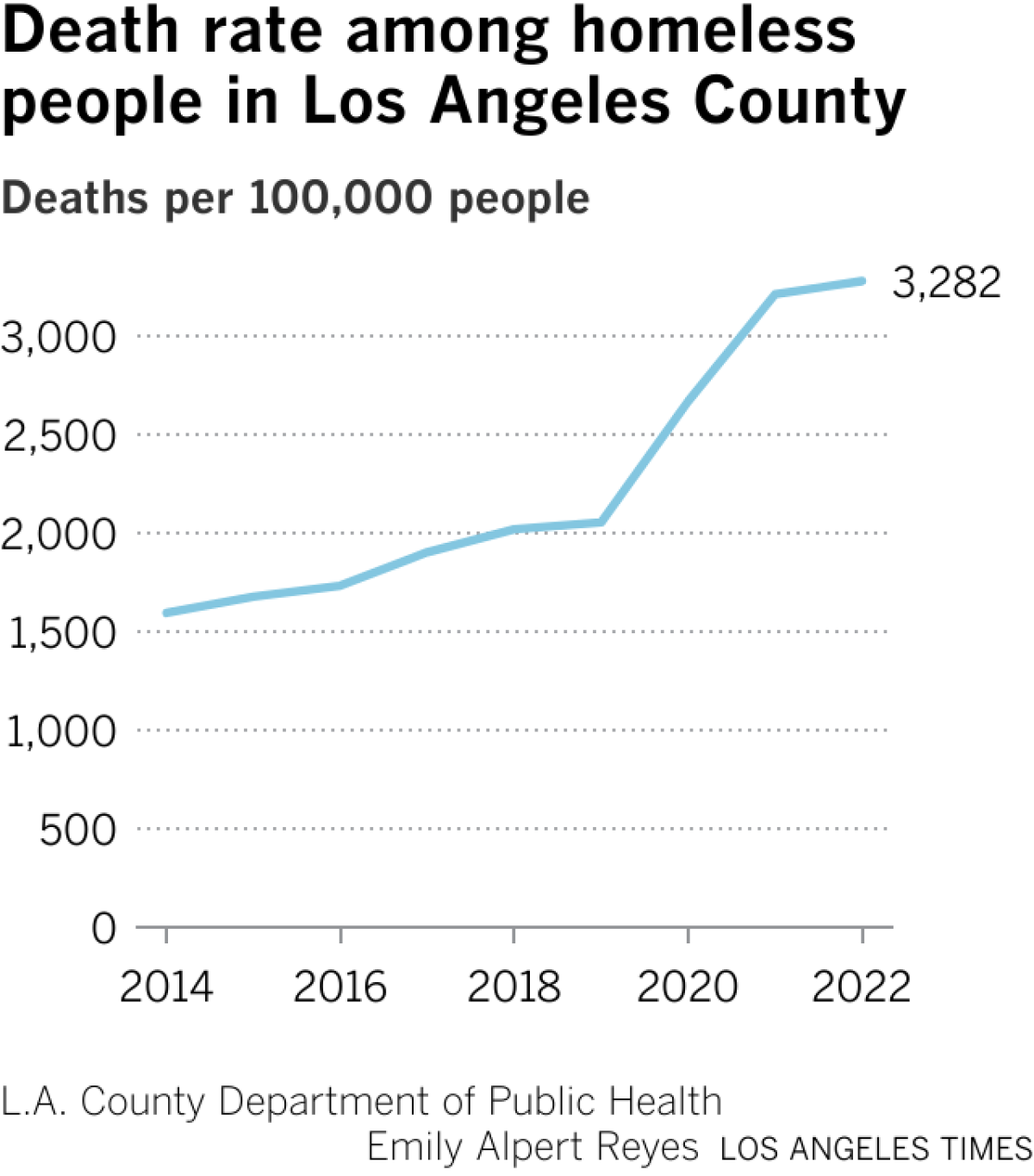
County officials said such efforts had also helped stabilize the death rate for homeless people overall after years of disturbing growth. As deadly overdoses stopped surging and COVID-19 deaths plunged, the overall mortality rate among unhoused people in L.A. County began to level off, the report found.
But homeless people remained far more likely than other county residents to die in a range of ways, including overdoses, traffic collisions, heart disease and homicide.
Their death rate overall was nearly four times higher than that of the broader population — a gap that has widened over time, public health officials found. And although it may have finally hit a plateau, the mortality rate for homeless people in L.A. County was still 60% higher than it had been three years earlier.
“This report highlights the continued need for concerted efforts to reduce the disproportionate burden of mortality among this vulnerable population,” L.A. County Public Health Director Barbara Ferrer said in a statement.
The county report also pointed out some alarming variations in the overall trends in L.A. County: For Black people who were unhoused, for instance, the rate of overdose deaths continued to rise significantly in 2022.
The rate of fatal overdoses also kept rising among homeless people in their 20s and 40s, the report found. That was offset by dropping rates among older people, but the report raised a grim possibility: After so many deadly years, “there may now be fewer surviving fentanyl and other opioid users over 50.”
Narcan can stop overdoses from opioids such as fentanyl, a powerful synthetic drug that has been involved in a rising share of overdose deaths among homeless people in L.A. County.
But fentanyl has not been the only threat: Roughly two-thirds of deadly overdoses among unhoused people involved more than one drug. Among the most commonly mingled were fentanyl and methamphetamine, a combination involved in nearly half of overdose deaths among homeless people in the county in 2022, according to the new report.
L.A. County public health officials called for a number of steps to bring down deaths among unhoused people, including expanding housing options so that people who use drugs will not lose their housing as a result; handing out more naloxone and test strips that detect fentanyl; and expanding preventative care for people who are homeless.

For the next five years, the Environmental Protection Agency has indicated it will not require public water utilities to test for microplastics or pharmaceuticals in drinking water, according to a proposed rule published in the Federal Register.
On Friday, the EPA submitted a list of chemicals it plans to test for under the Unregulated Contaminant Monitoring Rule, a mandatory testing program used to collect information about concerning chemicals in drinking water that could be harming human health. It did not include microplastics or pharmaceuticals.
The omissions come after announcements by EPA Administrator Lee Zeldin earlier this year that his agency was designating microplastics and pharmaceuticals priority contaminants for testing.
“This is a direct response to the concern of millions of Americans who have long demanded answers about what they and their families are drinking every day,” he said at an April news conference with Health and Human Secretary Robert F. Kennedy Jr. at EPA headquarters.
Zeldin’s announcement was seen at the time as a move to placate the increasingly disgruntled Make America Healthy Again contingent of Trump supporters.
Now the agency says it has no validated or standardized method to test for the plastic particles in drinking water, and wouldn’t be able to develop one before December, when testing is required to begin.
Among the 33 chemicals the EPA will require water utilities to test for are seven PFAS, or forever chemicals, and three pesticide residues.
It will be five years before the EPA proposes another list.
The EPA did not respond to a request for comment.
The agency noted in its proposed rule that it will collaborate with other federal agencies to “evaluate risks and exposures” of microplastics for future monitoring.
Environmentalists reacted with frustration and resignation. They pointed out that the European Union has developed methods to test for the tiny plastic particles, which have been found in people’s blood, brains and lung tissue. California has one in the works.
“The California water board has spent a lot of time and money on how to measure in drinking water,” said Judith Enck, a former EPA regional administrator and president of the anti-plastic environmental group Beyond Plastics. “EPA should give them a call.”
California was required by a 2018 state law to establish a protocol for local water utilities to test for the particles in drinking water. The state has not yet begun reporting its results, but protocols were established in 2021. Blair Robertson, a spokesman for the State Water Resources Control Board, said it’s not “a fully validated, end-to-end regulatory method” yet.
At the April meeting, Zeldin announced that he would place microplastics on what is known as the Contaminant Candidate List, which acts as a preliminary “watch list” of unregulated, priority contaminants in drinking water. Like the mandatory monitoring list, it is updated only every five years. The most recent list was published on April 2 — the day he made his announcement.
“Americans have been ignored as they sound the alarm about plastics in their drinking water,” Zeldin said during the announcement. “That ends today by placing microplastics on the contaminant candidate list for the first time ever. EPA will follow the science, will pursue answers and will hold ourselves to the highest standards to protect the health of Americans.”
There appears to be no clear association between these two lists, although the contaminant list is supposed to inform the monitoring list. Seventy-five chemicals and four chemical groups (microplastics, pharmaceuticals, PFAS chemicals, and disinfection byproducts) were listed on the 2026 contaminant list. Only seven of those chemicals were also on the proposed monitoring list (as well as seven PFAS chemicals).
When Zeldin announced microplastics as “‘a priority contaminant for regulation,’ and called it ‘a historic action on microplastics,’ he made it seem like the administration was going to take microplastics seriously,” said Mary Grant, water policy director for the environmental group Food & Water Watch.
“By not including them, they made it clear they don’t actually have plans to immediately address this crisis by getting the real-world monitoring data that we need right now to really start correcting ourselves,” she said.
Craig Davis, senior director of plastics chemistry at the American Chemistry Council — the nation’s largest trade group for chemical companies — said that while his organization supports microplastic research, it also agrees with the EPA’s decision not to include them in the monitoring list.
“National drinking water monitoring should be based on validated, standardized methods that can produce reliable and comparable data,” said Davis in a statement. He said “limited” national monitoring resources should be focused where data can produce “actionable public health information.”
The public has 60 days to comment once the plan is published in the Federal Register.

The number of Angelenos who went to the hospital with throat pain and concerns about smoke inhalation spiked as a fire burned through the massive Lineage cold storage warehouse in Boyle Heights this month, The Times has learned.
The blaze burned for eight days beginning June 17 and involved solar panels, insulation foam and other industrial materials.
During that time, more than three times as many people went to emergency departments within 10 miles of the warehouse mentioning the fire or smoke inhalation compared with the two weeks prior, according to data from the Los Angeles County Department of Public Health obtained through a public records request.
The agency also noted a near doubling of patients mentioning throat pain within five miles of the fire June 21 — 1.9 times the baseline levels.
Usually, fewer than 50 people go to the emergency room each day for throat pain, and fewer than 20 people for smoke inhalation, the department said.
The hospitalization data was tracked through the department’s syndromic surveillance project, which monitors trends in what people report when they come to emergency departments in L.A. County, as well as diagnosis codes noted by providers. The system is not as comprehensive as full patient health records, and clinicians may not always include key words about “fire,” “smoke” or other circumstantial information in their diagnoses, the public health department said.
As such, it “cannot capture the true number of [emergency department] visits related to symptoms from the fire and likely underestimates the true burden of fire related symptoms,” the department said.
Perhaps unexpectedly, the department said it did not note a substantial increase in asthma, acute respiratory symptoms or chronic obstructive pulmonary disease-related emergency department visits during the fire.
But even these preliminary findings are concerning, experts said. The fire is believed to have started on the solar array on the roof of the 500,000 square-foot building, which housed 85 million pounds of frozen food. It then reached an ammonia line, prompting two brief shelter-in-place orders for nearby residents.
Over the next week, the fire continued to burn through dense insulation foam within the building’s walls and other unknown industrial materials, blanketing much of L.A. in acrid smoke. Residents in downtown L.A., northeast L.A., Burbank, the San Gabriel Valley and many other parts of the city and county reported seeing and smelling the fumes.
The South Coast Air Quality Management District issued multiple warnings about unhealthy levels of PM 2.5, or fine particulate matter. The city and county opened two smoke respite shelters in the immediate area so that people could breath cleaner air.
It is still unclear what exactly was in the smoke that people breathed in. Industrial fires release far more materials than the burned wood smoke that is emitted during wildfires.
“The makeup of the smoke can include toxic chemicals, fine particles and other serious risks to lung health depending on fire conditions and what is burned,” Will Barrett, assistant vice president for nationwide clean air policy at the American Lung Assn., said as the fire was burning. Children and elderly people are particularly at risk.
David Eisenman, director of the UCLA Center for Public Health and Disasters, said urban industrial fires also can represent a hazard that standard PM 2.5 warnings don’t always address. Those advisories are “blunt instruments” that don’t adequately capture emissions from burning man-made goods — or convey that the source of pollution may include burning batteries or toxic refrigerants, he said.
The fact that initial numbers don’t show a spike in asthma attacks is “somewhat reassuring,” Eisenman said. But “people may have gone to their primary care doctors, which this would not capture. This data deserves follow up.”
The air district and the U.S. Environmental Protection Agency deployed air monitors to assess particulate matter, airborne toxic metals and other harmful compounds during the early days of the blaze. The air district said it didn’t find significant levels of air toxics during the first two days of the fire, although it did record significantly elevated concentrations of particulate matter within the plume downwind.
Some of the measurements it took with mobile monitors, which are five-minute snapshots, also showed increased bromine and chlorine, which often are found when buildings burn and were at levels “below short-term health-based exposure thresholds,” the air district said. It began continuous PM 2.5. monitoring at two nearby elementary schools on the third day.
The L.A. Fire Department said it detected low-levels of toxic hydrogen fluoride on the second day of the fire, which can be a byproduct of burning lithium-ion batteries.
Lineage, the tenant-operator of the warehouse, said no concentrations of ammonia were detected in the air at any time.
“There’s no doubt this fire has had a huge impact on the local community, and we are committed to showing up in every way we can,” company officials wrote in a statement last week. They said Lineage worked closely with the Fire Department during the blaze and delivered masks, air purifiers and other supplies to the community, and will work to ensure the fastest cleanup possible.
The long-term health effects of the fire and its smoke probably won’t be known unless researchers conduct a follow-up study, said Eisenman of UCLA.
For example, there may have been delayed pulmonary effects from the hydrogen fluoride and burning insulation foam that — when combined with the elevated PM 2.5 levels in a dense urban environment — produced health effects that didn’t show up in the emergency room data.
“They will show up in increased primary care office visits and exacerbations of chronic disease over the next few weeks,” he said. “So from a public health standpoint, this fire is not over.”

LOS ANGELES — All the water unleashed onto the warehouse fire in Boyle Heights — some of it 480 gallons at a time by helicopter — had to end up somewhere.
That somewhere is the Los Angeles River.
Los Angeles Fire Department crews ripped through 50-foot walls filled with foam insulation to get to the building’s steel skeleton and its storage racks.
Charred chunks of foam have been floating from the burn site, partially blocking storm drains. Now organizers from East Yard Communities for Environmental Justice are teaming up with scientists from UCLA and Columbia University to find out more about what’s in the runoff.
“The community here is really interested in knowing, ‘Are there any contaminants that are potentially making their way down to the L.A. River?’” said Yoshira “Yoshi” Ornelas Van Horne, UCLA assistant professor in environmental health sciences. “We really can’t answer that unless we actually have measures and samples analyzed.”
Water samples collected directly from the warehouse fire runoff have been shipped to Columbia‘s Multi-Element Trace Analysis Laboratory in New York, which has a spectrometer that can identify trace levels of elements. The lab also has relationships with researchers in Southern California.
2

1. Emmanuel Carrera Ruedas, left, and Casey Cooper prep containers to take water samples from the L.A. River. 2. Casey Cooper holds a water sample. (Christina House / Los Angeles Times)
The data will then come back to UCLA for analysis. For now, the scientists and community advocates only have the money to test for copper, lead and arsenic, Ornelas Van Horne said. Residents have expressed interest in testing for more contaminants.
As the water from the firefighting efforts trickles through the warehouse in rivulets, it forms a stream at the corner of S. Indiana and Noakes streets, that gushed into the storm drain. On a recent visit, the water traversed a smoky 10-foot canyon of charred foam and twisted wall panels on its way to the drain.
From there, the water flows to the L.A. River. Despite the fact that its concrete design is intended to whisk water out of the city as fast as possible, life stubbornly persists in the river and nearby. Recreational swimming is not permitted, yet anglers fishing for tilapia, largemouth bass and carp are a common sight along the rocky sides of the soft-bottom areas.
The L.A. River, and all it carries with it, meets the ocean in Long Beach.
The L.A. County Public Works Department said it has deployed three containment booms — floating barriers — on the L.A. River, and is continuing to monitor the water as it makes its way to the ocean.

Emmanuel Carrera Ruedas takes a water sample.
(Christina House / Los Angeles Times)
Before it gets there, the river passes through the Dominguez wetlands, where Public Works is removing some number of dead fish. The wetland has absorbed toxic runoff from a warehouse fire before, resulting in a fish die-off.
“For so long, the L.A. River has been used as a dumping ground for all kinds of chemicals,” said Emmanuel Carrera Ruedas, a community scientist and member of East Yard Communities for Environmental Justice.
Pollution has plagued the L.A. River, but it does have allies. In the 1980s, the Friends of the LA River pushed to address street runoff and trash that had made the water body infamous. Significant progress from advocacy and government initiatives improved water conditions, but these efforts have not been equally distributed.
Carrera said the samples represent “proof of what’s actually going on, and accountability, too, for the city, of not just what’s happening in our air, but what’s actually happening in our waterways.”
The first samples for the project were taken last Friday, the second day of the fire.
They were the first of 20 samples the research groups have agreed to test at no cost to see if any exceed regulatory standards and could pose a risk to people nearby.
The warehouse fire represents the latest environmental disaster for people in Boyle Heights and East L.A. Just four weeks ago, a telecommunications crew accidentally struck one of the many oil pipelines beneath the L.A. area, spilling 25,000 gallons of crude oil near Eastern and Cesar Chavez avenues — including into storm drains feeding to the L.A. River.
“I think it really is difficult to see disaster after disaster hit the communities here, with not a lot of talk about how we can move through these disasters together,” said Casey Cooper, a volunteer community scientist involved in the sampling. They were inspired, they said, by the response of neighbors, and how people were supporting one another.
Results from the laboratory analysis could be back to Ornelas Van Horne within a month.
-

 Nebraska5 minutes ago
Nebraska5 minutes agoErstad joins Nebraska golf program
-

 Nevada8 minutes ago
Nevada8 minutes ago‘Arrive Alive’ initiative with Nevada Department of Public Safety, FOX5
-

 New Hampshire13 minutes ago
New Hampshire13 minutes agoThis NH Short Film Festival Returns in July, and Every Film Clocks in at 15 Minutes or Less
-

 New Jersey20 minutes ago
New Jersey20 minutes agoNew Jersey’s $60.7 billion budget signed into law by Gov. Mikie Sherrill • The Jersey Vindicator
-

 New Mexico23 minutes ago
New Mexico23 minutes agoCommunity Champions: New Mexico’s Flo Valdez inducted into NFHS
-

 North Carolina28 minutes ago
North Carolina28 minutes agoNorth Carolina mail carrier kidnapped and killed while on her route, authorities say
-

 North Dakota35 minutes ago
North Dakota35 minutes agoJune ND severe weather recap: 5 tornadoes, damaging winds impact numerous towns
-

 Ohio38 minutes ago
Ohio38 minutes ago‘Pure evil’: Adults arrested after 16 children found in deplorable conditions in Ohio home

