Science
Faster alerts for California megaquakes: Early-warning system gets major upgrade

California’s earthquake early-warning system is getting a seismic upgrade, one that will allow residents to receive more timely alerts about shaking from an incoming megaquake.
The upgrade, also available in Oregon and Washington, will provide features important for warnings about the “Big One.”
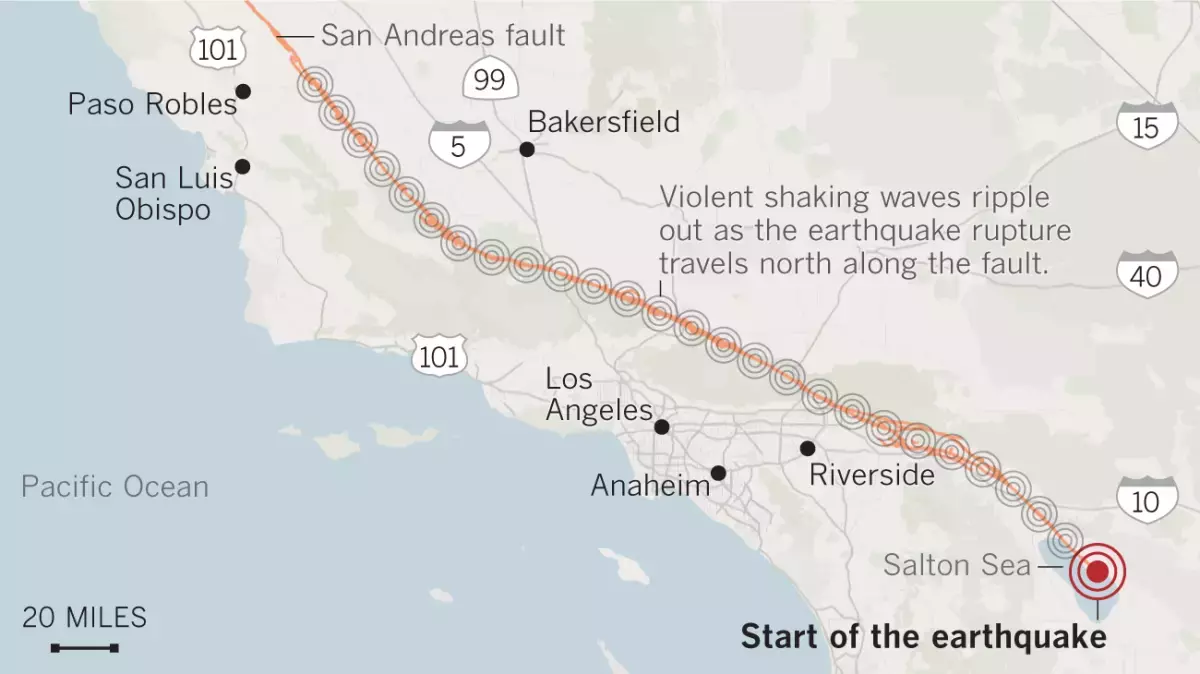
The improvements could mean that, depending on where they are and where the quake begins, Californians would receive an earlier, more accurate estimate of magnitude before the earth starts shaking — say from a magnitude 7.8 earthquake that begins on the San Andreas fault near the Mexican border and ruptures the fault toward Los Angeles County.
The upgrade also would improve warnings for the Pacific Northwest and California’s North Coast, which are threatened by tsunamis from quakes along the Cascadia subduction zone.
The U.S. Geological Survey and its nonprofit partner EarthScope announced the upgraded system Wednesday.
For the most powerful earthquakes, the improvements “become very, very critical in helping us get to the answer quicker — in terms of how big that event is,” said Robert de Groot, one of the operations team leaders of the USGS’ ShakeAlert System.
For smaller earthquakes, the older system worked “perfectly fine,” De Groot said. But with larger quakes, the magnitude could be underestimated for quite some time, robbing residents of crucial information in the seconds before they feel the most destructive shaking.
Let’s say an earthquake on the southern San Andreas fault that starts near the Mexican border ends up being a magnitude 8, but the earliest estimate says it’s a magnitude 6.5. The longer that underestimate is broadcasting to phones, the less likely people are to take appropriate action.
“People would react differently — much differently — than if you said it was a magnitude 8,” said David Mencin, vice president of data services for EarthScope, a nonprofit funded by the National Science Foundation, USGS and NASA that’s supplying data for the improved early-warning system.
“The largest, most destructive earthquakes are the ones that we’re really worried about,” Mencin said. “This fixes the problem of underestimating those magnitudes, which is critical.”
One of the most famous underestimations came in 2011 with the epic magnitude 9.1 earthquake that triggered a devastating tsunami off the eastern coast of Japan, leaving roughly 18,000 dead. An initial estimate put the quake’s magnitude at 7.9, meaning the actual earthquake was an astonishing 63 times stronger in terms of energy released.
That underestimation led to a misjudgment of tsunami heights — with some of the first detailed alerts erroneously estimating the tsunami would be lower than protective sea walls. And when communications were cut off, a false sense of security settled in, with many people never receiving accurate evacuation alerts.
Had Japan used GPS data, a more accurate magnitude of the quake could’ve been generated far more quickly, Mencin said.
The USGS’ West Coast earthquake early-warning system has long relied on hundreds of seismic sensors embedded in the ground. But there is only so much shaking they can detect in a short time.
“Seismometers tend to get overwhelmed for earthquakes that are magnitude 7 and greater. They can begin to get ‘saturated,’” Mencin said. During particularly intense shaking, the seismometers — basically objects on a spring — start to hit the wall of the instrument, and so the seismic signal is “clipped” and can’t quickly calculate magnitudes above a certain threshold.
Coming to the rescue now are hundreds of GPS sensors on Earth’s surface and run by EarthScope. Most of the time, these sensors track very slow movement, on the order of millimeters or less per year. That can illustrate subtle tectonic plate action between major earthquakes, illustrating how the Pacific plate, where L.A. is located, is nudging northwest relative to the North American plate, where the Mojave Desert is located.
But in a major earthquake, there is considerable, permanent movement of the ground, where one piece of land jolts away from the other, moving yards in seconds. In the great San Francisco earthquake of 1906, land on one side of the San Andreas fault generally jammed 8.5 feet past the other, De Groot said.
And in the last great southern San Andreas earthquake — rupturing the fault in 1857 between Monterey and San Bernardino counties — land on one side of the fault generally lurched 10 feet relative to the other side. Both the 1857 and 1906 earthquakes were somewhere around magnitude 7.8.
In the largest of the Ridgecrest earthquakes in 2019, there were about 2 feet of fault offset for the magnitude 7.1 quake, De Groot said.
The first calculation of the earthquake early-warning system will still rely on seismic sensors, which measure ground velocity and acceleration, De Groot said. Then, as a quake continues to rupture along a fault, GPS sensors will measure the distance a block of land has moved.
“What GPS allows us to do is to get a handle on how big that earthquake is getting — or could be — sooner,” De Groot said. That means the early-warning system could realize a quake was a magnitude 7, or higher, a few seconds earlier than before.
It’s important to know that an earthquake’s magnitude doesn’t appear instantly. Quakes rupture on a fault at the speed of sound through rock, which is slower than the light speed of today’s telecommunications systems. This is the principle that allows people farther away from the start of an earthquake to get seconds of advance warning of the worst shaking to come.
On the San Andreas fault, an earthquake that begins rupturing at the Salton Sea and ends at Mt. San Gorgonio, roughly 80 miles away, would produce a magnitude 7.3 earthquake.
A rupture of the San Andreas fault between the Salton Sea and Mt. San Gorgonio could produce a magnitude 7.3 quake.
(Angelica Quintero / Los Angeles Times)
But one that ruptures the entire 340-mile length of the southern San Andreas, ending in Monterey County, would create a magnitude 8.2 earthquake and produce shaking over a much wider swath of Southern and Central California.
A rupture of the entire 340-mile length of the southern San Andreas fault between Monterey County and the Salton Sea would produce a magnitude 8.2 earthquake.
(Angelica Quintero / Los Angeles Times)
“As the earthquake grows in size, it’ll be able to help update that magnitude more quickly and with more accuracy,” De Groot said of the GPS data, which will spread the early warnings to a larger region. “By adding in the [GPS] data, you actually get a handle on how big the earthquake really is sooner.”
The net result will “translate into longer warning times for people who could potentially get alerts on their phones,” De Groot said. That would give people more time to take action, such as surgeons and dentists moving sharp tools from near patients, allowing trains to slow to reduce the risk of derailment, opening firehouse doors before they can be jammed shut and giving the public time to drop, cover and hold on.
Depending on where people are, some may not get a warning before they feel the first shaking, which is known as the “P wave.” But the goal is to give a warning before the most damaging shaking occurs — the “S wave” — which comes later.
“What we really want to get people to know about is getting the alert before the strongest shaking,” De Groot said.
By the end of 2025, the USGS’ ShakeAlert — which is about 90% complete — is expected to have 1,675 seismic sensing stations. EarthScope says an additional 1,000 GPS stations run by the nonprofit are contributing data to the system.
EarthScope, the nation’s primary seismological and geodetic data facility, was recently formed as the merger of UNAVCO, which held an archive for GPS data, and IRIS, which held a seismic data archive.
The earthquake early-warning system has become more popular in recent years as people get more accustomed to the alerts. In February’s widely felt magnitude-4.6 earthquake in Malibu, some felt left out when they didn’t receive an early warning.
The alerts can be received by downloading the free MyShake app on iOS and Android. Android users are automatically subscribed to Android Earthquake Alerts. Those systems are set to sound an alarm when an earthquake is estimated to be of magnitude 4.5 or higher and the expected shaking intensity at the user’s cellphone location is expected to be at least “weak” — level 3 on the Modified Mercalli Intensity Scale, where it’s felt quite noticeably by people indoors and may rock standing motor vehicles slightly or feel like a truck is passing by.
Earthquakes of greater strength — magnitude 5 and above — will send users a wireless emergency alert, similar to an Amber Alert, if they’re in a location expected to get at least “light” shaking intensity. That’s level 4 on the Modified Mercalli Intensity Scale — shaking intensity enough to rattle dishes, windows and doors, and can feel like a heavy truck striking a building.








Central Coast Water authorities approved waste discharge permits for Diablo Canyon nuclear plant Thursday, making it nearly certain it will remain running through 2030, and potentially through 2045.
The Pacific Gas & Electric-owned plant was originally supposed to shut down in 2025, but lawmakers extended that deadline by five years in 2022, fearing power shortages if a plant that provides about 9 percent the state’s electricity were to shut off.
In December, Diablo Canyon received a key permit from the California Coastal Commission through an agreement that involved PG&E giving up about 12,000 acres of nearby land for conservation in exchange for the loss of marine life caused by the plant’s operations.
Today’s 6-0 vote by the Central Coast Regional Water Board approved PG&E’s plans to limit discharges of pollutants into the water and continue to run its “once-through cooling system.” The cooling technology flushes ocean water through the plant to absorb heat and discharges it, killing what the Coastal Commission estimated to be two billion fish each year.
The board also granted the plant a certification under the Clean Water Act, the last state regulatory hurdle the facility needed to clear before the federal Nuclear Regulatory Commission (NRC) is allowed to renew its permit through 2045.
The new regional water board permit made several changes since the last one was issued in 1990. One was a first-time limit on the chemical tributyltin-10, a toxic, internationally-banned compound added to paint to prevent organisms from growing on ship hulls.
Additional changes stemmed from a 2025 Supreme Court ruling that said if pollutant permits like this one impose specific water quality requirements, they must also specify how to meet them.
The plant’s biggest water quality impact is the heated water it discharges into the ocean, and that part of the permit remains unchanged. Radioactive waste from the plant is regulated not by the state but by the NRC.
California state law only allows the plant to remain open to 2030, but some lawmakers and regulators have already expressed interest in another extension given growing electricity demand and the plant’s role in providing carbon-free power to the grid.
Some board members raised concerns about granting a certification that would allow the NRC to reauthorize the plant’s permits through 2045.
“There’s every reason to think the California entities responsible for making the decision about continuing operation, namely the California [Independent System Operator] and the Energy Commission, all of them are sort of leaning toward continuing to operate this facility,” said boardmember Dominic Roques. “I’d like us to be consistent with state law at least, and imply that we are consistent with ending operation at five years.”
Other board members noted that regulators could revisit the permits in five years or sooner if state and federal laws changes, and the board ultimately approved the permit.

The H5N1 bird flu virus that devastated South American elephant seal populations has been confirmed in seals at California’s Año Nuevo State Park, researchers from UC Davis and UC Santa Cruz announced Wednesday.
The virus has ravaged wild, commercial and domestic animals across the globe and was found last week in seven weaned pups. The confirmation came from the U.S. Department of Agriculture’s National Veterinary Services Laboratory in Ames, Iowa.
“This is exceptionally rapid detection of an outbreak in free-ranging marine mammals,” said Professor Christine Johnson, director of the Institute for Pandemic Insights at UC Davis’ Weill School of Veterinary Medicine. “We have most likely identified the very first cases here because of coordinated teams that have been on high alert with active surveillance for this disease for some time.”
Since last week, when researchers began noticing neurological and respoiratory signs of the disease in some animals, 30 seals have died, said Roxanne Beltran, a professor of ecology and evolutionary biology at UC Santa Cruz. Twenty-nine were weaned pups and the other was an adult male. The team has so far confirmed the virus in only seven of the dead pups.
Infected animals often have tremors convulsions, seizures and muscle weakness, Johnson said.
Beltran said teams from UC Santa Cruz, UC Davis and California State Parks monitor the animals 260 days of the year, “including every day from December 15 to March 1” when the animals typically come ashore to breed, give birth and nurse.
The concerning behavior and deaths were first noticed Feb. 19.
“This is one of the most well-studied elephant seal colonies on the planet,” she said. “We know the seals so well that it’s very obvious to us when something is abnormal. And so my team was out that morning and we observed abnormal behaviors in seals and increased mortality that we had not seen the day before in those exact same locations. So we were very confident that we caught the beginning of this outbreak.”
In late 2022, the virus decimated southern elephant seal populations in South America and several sub-Antarctic Islands. At some colonies in Argentina, 97% of pups died, while on South Georgia Island, researchers reported a 47% decline in breeding females between 2022 and 2024. Researchers believe tens of thousands of animals died.
More than 30,000 sea lions in Peru and Chile died between 2022 and 2024. In Argentina, roughly 1,300 sea lions and fur seals perished.
At the time, researchers were not sure why northern Pacific populations were not infected, but suspected previous or milder strains of the virus conferred some immunity.
The virus is better known in the U.S. for sweeping through the nation’s dairy herds, where it infected dozens of dairy workers, millions of cows and thousands of wild, feral and domestic mammals. It’s also been found in wild birds and killed millions of commercial chickens, geese and ducks.
Two Americans have died from the virus since 2024, and 71 have been infected. The vast majority were dairy or commercial poultry workers. One death was that of a Louisiana man who had underlying conditions and was believed to have been exposed via backyard poultry or wild birds.
Scientists at UC Santa Cruz and UC Davis increased their surveillance of the elephant seals in Año Nuevo in recent years. The catastrophic effect of the disease prompted worry that it would spread to California elephant seals, said Beltran, whose lab leads UC Santa Cruz’s northern elephant seal research program at Año Nuevo.
Johnson, the UC Davis researcher, said the team has been working with stranding networks across the Pacific region for several years — sampling the tissue of birds, elephant seals and other marine mammals. They have not seen the virus in other California marine mammals. Two previous outbreaks of bird flu in U.S. marine mammals occurred in Maine in 2022 and Washington in 2023, affecting gray and harbor seals.
The virus in the animals has not yet been fully sequenced, so it’s unclear how the animals were exposed.
“We think the transmission is actually from dead and dying sea birds” living among the sea lions, Johnson said. “But we’ll certainly be investigating if there’s any mammal-to-mammal transmission.”
Genetic sequencing from southern elephant seal populations in Argentina suggested that version of the virus had acquired mutations that allowed it to pass between mammals.
The H5N1 virus was first detected in geese in China in 1996. Since then it has spread across the globe, reaching North America in 2021. The only continent where it has not been detected is Oceania.
Año Nuevo State Park, just north of Santa Cruz, is home to a colony of some 5,000 elephant seals during the winter breeding season. About 1,350 seals were on the beach when the outbreak began. Other large California colonies are located at Piedras Blancas and Point Reyes National Sea Shore. Most of those animals — roughly 900 — are weaned pups.
It’s “important to keep this in context. So far, avian influenza has affected only a small proportion of the weaned at this time, and there are still thousands of apparently healthy animals in the population,” Beltran said in a press conference.
Public access to the park has been closed and guided elephant seal tours canceled.
Health and wildlife officials urge beachgoers to keep a safe distance from wildlife and keep dogs leashed because the virus is contagious.

Kate Movius moved among a roomful of Los Angeles County sheriff’s deputies, passing out a pop trivia quiz and paper prism glasses.
She told them to put on the vision-distorting glasses, and to write with their nondominant hand. As they filled out the tests, Movius moved about the City of Industry classroom pounding abruptly on tables. Then came the cowbell. An aide flashed the overhead lights on and off at random. The goal was to help the deputies understand the feeling of sensory overwhelm, which many autistic people experience when incoming stimulation exceeds their capacity to process.
“So what can you do to assist somebody, or de-escalate somebody, or get information from someone who suffers from a sensory disorder?” Movius asked the rattled crowd afterward. “We can minimize sensory input. … That might be the difference between them being able to stay calm and them taking off.”
Movius, founder of the consultancy Autism Interaction Solutions, is one of a growing number of people around the U.S. working to teach law enforcement agencies to recognize autistic behaviors and ensure that encounters between neurodevelopmentally disabled people and law enforcement end safely.
She and City of Industry Mayor Cory Moss later passed out bags filled with tools donated by the city to aid interactions: a pair of noise-damping headphones to decrease auditory input, a whiteboard, a set of communication cards with words and images to point to, fidget toys to calm and distract.
“The thing about autistic behavior when it comes to law enforcement is a lot of it may look suspicious, and a lot of it may feel very disrespectful,” said Movius, who is also the parent of an autistic 25-year-old man. Responding officers, she said, “are not coming in thinking, ‘Could this be a developmentally disabled person?’ I would love for them to have that in the back of their minds.”
A sheriff’s deputy reads a pamphlet on autism during the training program.
(Genaro Molina / Los Angeles Times)
Autism spectrum disorder is a developmental condition that manifests differently in nearly every person who has it. Symptoms cluster around difficulties in communication, social interaction and sensory processing.
An autistic person stopped by police might hold the officer’s gaze intensely or not look at them at all. They may repeat a phrase from a movie, repeat the officer’s question or temporarily lose their ability to speak. They might flee.
All are common involuntary responses for an autistic person in a stressful situation, which a sudden encounter with law enforcement almost invariably is. To someone unfamiliar with the condition, all could be mistaken for intoxication, defiance or guilt.
Autism rates in the U.S. have increased nearly fivefold since the Centers for Disease Control began tracking diagnoses in 2000, a rise experts attribute to broadening diagnostic criteria and better efforts to identify children who have the condition.
The CDC now estimates that 1 in 31 U.S. 8-year-olds is autistic. In California, the rate is closer to 1 in 22 children.
As diverse as the autistic population is, people across the spectrum are more likely to be stopped by law enforcement than neurotypical peers.
About 15% of all people in the U.S. ages 18 to 24 have been stopped by police at some point in their lives, according to federal data. While the government doesn’t track encounters for disabled people specifically, a separate study found that 20% of autistic people ages 21 to 25 have been stopped, often after a report or officer observation of a person behaving unusually.
Some of these encounters have ended in tragedy.
In 2021, Los Angeles County sheriff’s deputies shot and permanently paralyzed a deaf autistic man after family members called 911 for help getting him to a hospital.
Isaias Cervantes, 25, had become distressed about a shopping trip and started pushing his mother, his family’s attorney said at the time. He resisted as two deputies attempted to handcuff him and one of the deputies shot him, according to a county report.
In 2024, Ryan Gainer’s family called 911 for support when the 15-year-old became agitated. Responding San Bernardino County sheriff‘s deputies shot and killed him outside his Apple Valley home.
Last year, police in Pocatello, Idaho, shot Victor Perez, 17, through a chain-link fence after the nonspeaking teenager did not heed their shouted commands. He died from his injuries in April.

Sheriff’s deputies take a trivia quiz using their non-writing hands, while wearing vision-distorting glasses, as Kate Movius, standing left, and Industry Mayor Cory Moss, right, ring cowbells. The idea was to help them understand the sensory overwhelm some autistic people experience.
(Genaro Molina / Los Angeles Times)
As early as 2001, the FBI published a bulletin on police officers’ need to adjust their approach when interacting with autistic people.
“Officers should not interpret an autistic individual’s failure to respond to orders or questions as a lack of cooperation or as a reason for increased force,” the bulletin stated. “They also need to recognize that individuals with autism often confess to crimes that they did not commit or may respond to the last choice in a sequence presented in a question.”
But a review of multiple studies last year by Chapman University researchers found that while up to 60% of officers have been on a call involving an autistic person, only 5% to 40% had received any training on autism.
In response, universities, nonprofits and private consultants across the U.S. have developed curricula for law enforcement on how to recognize autistic behaviors and adapt accordingly.
The primary goal, Movius told deputies at November’s training session, is to slow interactions down to the greatest extent possible. Many autistic people require additional time to process auditory input and verbal responses, particularly in unfamiliar circumstances.
If at all possible, Movius said, wait 20 seconds for a response after asking a question. It may feel unnaturally long, she acknowledged. But every additional question or instruction fired in that time — what’s your name? Did you hear me? Look at me. What’s your name? — just decreases the likelihood that a person struggling to process will be able to respond at all.
Moss’ son, Brayden, then 17, was one of several teenagers and young adults with autism who spoke or wrote statements to be read to the deputies. The diversity of their speech patterns and physical mannerisms showed the breadth of the spectrum. Some were fluently verbal, while others communicated through signs and notes.
“This population is so diverse. It is so complicated. But if there’s anything that we can show [deputies] in here that will make them stop and think, ‘Hey, what if this is autism?’ … it is saving lives,” Moss said.

Mayor Cory Moss, left, and Kate Movius hug at the end of the training program last November. Movius started Autism Interaction Solutions after her son was born with profound autism.
(Genaro Molina / Los Angeles Times)
Some disability advocates cautioned that it takes more than isolated training sessions to ensure encounters end safely.
Judy Mark, co-founder and president of the nonprofit Disability Voices United, says she trained thousands of officers on safe autism interactions but stopped after Cervantes’ shooting. She now urges families concerned about an autistic child’s safety to call an ambulance rather than law enforcement.
“I have significant concern about these training sessions,” Mark said. “People get comfort from it, and the Sheriff’s Department can check the box.”
While not a panacea, supporters argue that a brief course is better than no preparation at all. Some years ago, Movius received a letter from a man whose profoundly autistic son slipped away as the family loaded their car at the beach. He opened the unlocked door of a police vehicle, climbed into the back and began to flail in distress.
Though surprised, the officer seated at the wheel de-escalated the situation and helped the young man find his family, the father wrote to Movius. He had just been to her training.

Soccer Frenzy: Cities, Fans, and What to Know | Futbol HQ

Fan behind Anthony Edwards’ orange bracelet has beaten cancer

New bridge over 96th Street adds to Nickel Plate Trail connections

Pittsburgh International’s T. rex could soon disappear from view

Popn’ Off Gourmet Popcorn opens on Broad Street in Augusta

Florida High School Football Rankings: Top 25 teams – Oct. 21

Cleary's 21 help Le Moyne down Central Connecticut State 69-64 in OT

How old is Bo Nix? What to know about Oregon quarterback ahead of 2024 NFL Draft

99th annual Pony Swim held in Virginia

Indiana Members Credit Union announced as new anchor tenant at Bottleworks District

Where Iran’s ballistic missiles can reach — and how close they are to the US

Has India’s influence in Afghanistan grown under the Taliban?

Bill Clinton to testify before House committee investigating Epstein links

Read Judge Schiltz’s Order

Vulnerable House Dem lashes out at Trump’s ‘racist’ SOTU challenge: ‘That was uncomfortable’
-

 World2 days ago
World2 days agoExclusive: DeepSeek withholds latest AI model from US chipmakers including Nvidia, sources say
-

 Massachusetts2 days ago
Massachusetts2 days agoMother and daughter injured in Taunton house explosion
-

 Montana1 week ago
Montana1 week ago2026 MHSA Montana Wrestling State Championship Brackets And Results – FloWrestling
-

 Oklahoma1 week ago
Oklahoma1 week agoWildfires rage in Oklahoma as thousands urged to evacuate a small city
-

 Louisiana5 days ago
Louisiana5 days agoWildfire near Gum Swamp Road in Livingston Parish now under control; more than 200 acres burned
-

 Denver, CO2 days ago
Denver, CO2 days ago10 acres charred, 5 injured in Thornton grass fire, evacuation orders lifted
-

 Technology6 days ago
Technology6 days agoYouTube TV billing scam emails are hitting inboxes
-

 Technology6 days ago
Technology6 days agoStellantis is in a crisis of its own making