Science
U.S. death toll tied to long COVID exceeds 4,000, CDC report says
The well being challenges {that a} bout of COVID-19 generally leaves in its wake may be troublesome, scary and fairly mysterious. New analysis confirms they are often lethal as effectively.
A examine launched Wednesday by the Facilities for Illness Management and Prevention discovered that between January 2020 and June 2022, lengthy COVID was implicated in not less than 3,544 deaths in the US alone.
The authors of the examine acknowledge that their tally of lengthy COVID fatalities is probably going a major undercount of individuals whose deaths have been brought on, not less than partially, by COVID-19’s lingering results. It represents a mere sliver — lower than 0.4% — of the greater than 1 million pandemic deaths that occurred in the course of the examine interval in the US.
However the brand new analysis contributes to mounting proof that COVID-19’s toll doesn’t all the time finish with a unfavourable check. And it means that for a lot of sufferers, new signs of poor well being — from nervousness and sleep difficulties to coronary heart arrhythmias and blood clots — could have unrecognized roots in a earlier coronavirus an infection.
Generally, these signs stem from infections sufferers didn’t even know they’d.
“Viruses have long-term penalties,” stated Dr. Ziyad Al-Aly, a doctor with the Veterans Affairs St. Louis Well being Care System who has studied the downstream well being results of an encounter with the SARS-CoV-2 virus.
“We’re fairly good at capturing acute illness,” he added. However researchers and medical professionals have a “main, main blind spot” with regards to anticipating and detecting the longer-term fallout of a viral an infection, he stated.
Al-Aly, who was not concerned within the new CDC analysis, teaches epidemiology at Washington College in St. Louis. He led a current examine that detected sharp will increase in 20 cardiovascular diagnoses in sufferers in the course of the 12 months that adopted an an infection with the virus that causes COVID.
The CDC report affords “a gross underestimate” of the deaths possible attributable to lengthy COVID, Al-Aly stated. However, he added, it makes clear that with extra consciousness and a greater accounting system, researchers might start to know how typically viral infections sow the seeds of future afflictions.
For a lot of the interval coated by the brand new examine, the lingering well being results of COVID-19 weren’t a well-defined syndrome. Scientists have come to comprehend it as post-acute sequelae of COVID, or PASC, and the federal authorities launched a program to check it in February 2021.
In October 2021, the U.S. authorities created a singular medical code to establish PASC in medical information. However the reason for PASC’s wide-ranging signs steadily goes unrecognized, and U.S. medical doctors nonetheless don’t uniformly use the figuring out medical code.
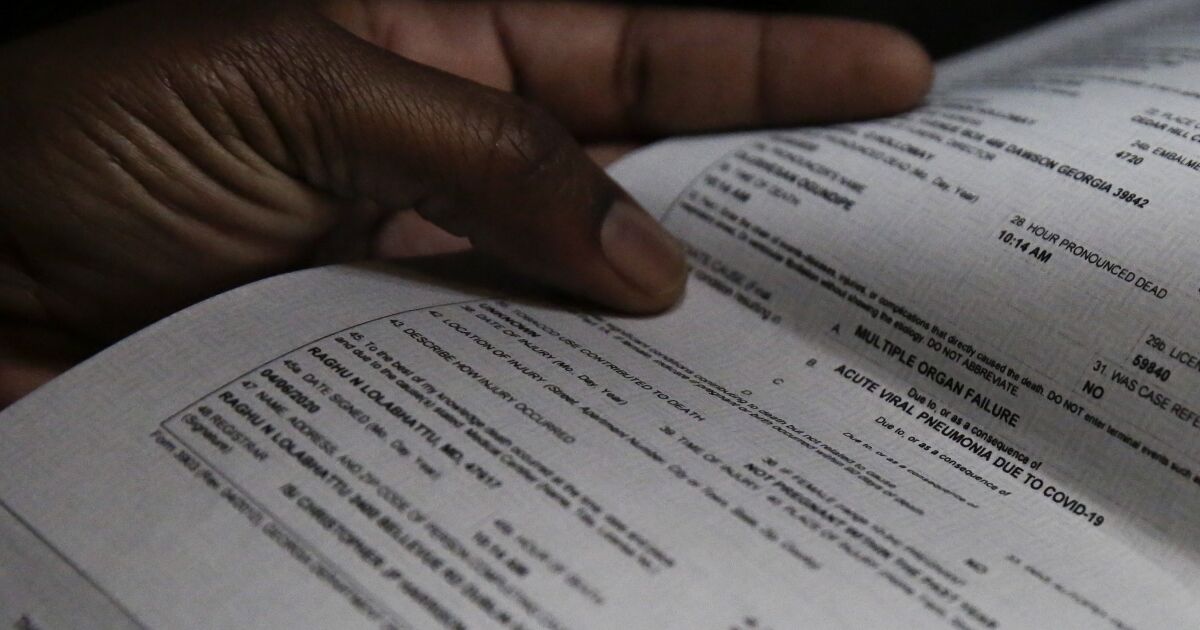
So to seize deaths wherein PASC possible performed a contributing function, researchers from the CDC’s Nationwide Middle for Well being Statistics needed to hunt for clues buried within the language of demise certificates. They began with 1,021,487 U.S. demise certificates that indicated COVID-19 as the first trigger. Then they scanned every for references to “persistent COVID,” “lengthy COVID,” “long-haul COVID” or “post-COVID syndrome” — all phrases which were extensively used to explain the motley set of afflictions some sufferers skilled after they’d apparently recovered from the illness.
An actual description of PASC — which most medical professionals now discuss with lengthy COVID — continues to evolve. Its hallmark signs are fatigue, cough, chest ache or shortness of breath, muscle weak point, mind fog, palpitations, and nervousness or melancholy.
The World Well being Group stories that about 1 in 4 individuals who have had COVID-19 proceed to expertise not less than one symptom a month after prognosis, and that roughly 1 in 10 have persistent signs after 12 weeks. In the US, 7.5% of people that stated they’d COVID-19 reported lingering results three months after recovering.
Scientists are racing to know lengthy COVID’s trigger. One surmise is that the syndrome is attributable to residual viral particles that continues to activate and/or exhaust the immune system. One other attributes it to virus that hides and replicates undetected in organs the place the immune system can’t get to it. The only clarification — {that a} case of extreme COVID-19 does lasting hurt to organs — doesn’t account for why individuals who have been scarcely in poor health generally wind up with lengthy COVID.
The brand new analysis discovered {that a} post-infection spiral towards demise was most readily detected in older individuals: Simply over 78% of the demise certificates that listed lengthy COVID as a attainable contributor have been for sufferers 65 and older.
Whereas ladies are thought to develop lengthy COVID extra steadily than males, the examine discovered demise certificates citing lengthy COVID have been barely extra prone to title males (51.5%) than ladies (48.5%).
Over the course of the pandemic, the listing of organs that could possibly be affected by COVID grew, yielding an image of a virus that traveled effectively past the lungs and higher respiratory system. Likewise, lengthy COVID could also be discovered to have an effect on a good wider vary of organs as analysis proceeds.
Cardiovascular issues have already appeared on each expanded lists. A number of months into the pandemic, medical doctors and scientists started to acknowledge that the coronavirus was inflicting blood clots, resulting in strokes, coronary heart assaults and emboli.
The examine by Al-Aly and his colleagues confirmed that, within the interval from one to 12 months after sufferers recovered from COVID-19, they’d an elevated threat for a variety of cardiovascular issues.
In comparison with an identical group of sufferers who had not had COVID-19, those that had have been 52% extra prone to endure a stroke and 66% extra prone to endure some type of blockage in blood circulation to the guts, together with one which ends in a coronary heart assault. As well as, former COVID sufferers have been 69% extra possible than unaffected friends to develop some type of coronary heart arrhythmia.
Not surprisingly, individuals who had been hospitalized with COVID have been extra prone to endure cardiovascular problems. However even sufferers whose brush with the coronavirus was gentle confronted an elevated threat. And whereas these over 65 have been most certainly to develop these problems, youthful and more healthy sufferers noticed their dangers rise too.


One of the best diets for health keeps getting better.
A new study that tracked more than 25,000 women for a quarter century found that the more their eating patterns were in sync with the Mediterranean diet, the less likely they were to die during that period. The relationship held up even when researchers accounted for other factors that influence longevity, including age, exercise habits and smoking history.
The findings were published Friday in the journal JAMA Network Open.
The Mediterranean diet is heavy on fruits, vegetables and whole grains. Extra virgin olive oil, which is rich in antioxidants, is the main source of fat. Protein comes from lean sources like beans, legumes and nuts as well as fish, poultry, eggs and low-fat or fat-free dairy. Wine is welcome in low to moderate amounts, while red and processed meats, butter and sweets are eaten sparingly or not at all.
The diet is a longtime favorite of doctors, nutritionists and weight-loss programs. Studies consistently show that it helps people slim down, reduce cholesterol and lower their blood pressure, all of which reduce the risk of cardiovascular disease. It also helps people manage their blood sugar and stave off Type 2 diabetes.
How, exactly, does the Mediterranean diet pull this off? That’s what Shafqat Ahmad, who studies cardiovascular disease development at Sweden’s Uppsala University and Harvard Medical School, and his colleagues wanted to find out.
They turned to the Women’s Health Study, which enrolled tens of thousands of female health professionals who were at least 45 years old. When the women joined the study in the mid-1990s, they answered 131 questions about the foods they ate.
The researchers used those answers to give each woman a score between 0 and 9 that reflected the degree to which they were following the Mediterranean diet. If they were above the median when it came to consumption of vegetables, fruits, nuts, whole grains, legumes or fish, they got one point. Ditto if they were above the median on their ratio of monounsaturated (which are good) to saturated (which are bad) fatty acids.
If the women were below the median for consumption of red and processed meats, they earned another point. And if they consumed between 5 and 15 grams of alcohol per day — the equivalent of a typical glass of wine or a can of beer — they got a point as well.
Those with total scores between 0 and 3 were categorized as having “low” adherence to the Mediterranean diet. A total of 4 or 5 was classified as “intermediate,” and a sum between 6 and 9 was considered “high.”
The Women’s Health Study ended in 2004, but researchers kept checking in with the participants once a year. Ahmad and his colleagues focused on the 25,315 women who had both diet data and a host of biomedical measurements from when they entered the study.
By November 2023, 3,879 of the women had died. But the risk of being among them wasn’t the same for everyone.
Compared to the women in the low adherence group, those in the intermediate group were 16% less likely to die during the study period, while the risk of death for those with the highest fidelity to the Mediterranean diet was 23% lower, according to the study.
When the researchers controlled for smoking behavior, physical activity, alcohol intake and menopausal factors, women in the intermediate group had an 8% lower risk of death, and those in the high group had an 11% lower risk of death.
In addition to a reduced risk of death from any cause, following the Mediterranean diet was associated with a lower risk of dying of cancer or cardiovascular disease, said Dr. Samia Mora, a cardiologist at Brigham and Women’s Hospital in Boston and the study’s senior author.
As for why the Mediterranean diet seemed to protect against premature death, the most influential factor — among the roughly 40 biomarkers the researchers could test — was a group of metabolites that appeared to explain 14.8% of the benefit. Ahmad and his colleagues called particular attention to higher levels of a useful amino acid called alanine as well as lower levels of another amino acid called homocysteine that is elevated in people with heart disease.
Inflammation accounted for 13% of the mortality benefit enjoyed by those with high adherence to the Mediterranean diet. Chronic inflammation is associated with a variety of health problems, including cardiovascular diseases, diabetes and some cancers.
A woman’s body mass index and a measure of how well her body processes triglycerides were each responsible for 10.2% of the reduced risk of death, and insulin resistance accounted for 7.4%.
The study suggests that making even modest improvements in these factors could help people get more longevity out the Mediterranean diet, Ahmad said.
But he and Mora added that there must be other biological mechanisms at work that their study wasn’t able to measure. The gut microbiome may be one of them, they said.
Dr. Frank Hu, a professor of nutrition and epidemiology at the Harvard T.H. Chan School of Public Health, said the study offers “new insights” into why people who embrace the Mediterranean diet tend to live longer.
“It suggests that the health benefits in reducing mortality are explained by its effects on harmful blood metabolites, inflammation, insulin resistance, and body weight rather than by reducing total and LDL cholesterol,” said Hu, who wasn’t involved in the work.
The study comes with several caveats, including the fact that 96% of the participants were white women. That means the results may not generalize to the population at large.
In addition, the women were asked about their eating habits only once, so there’s no way to know whether their diets changed as they got older.
However, Mercedes Sotos Pietro, a nutritional epidemiologist at the Autonomous University of Madrid, said the findings about the reduced risk of death are in line with research she has conducted using data from the Nurses Health Study and the Health Professionals Follow-up Study that assessed diet multiple times.
Sotos Pietro, who didn’t work on the new study, said the Mediterranean diet is “golden” because it includes a variety of tasty foods and doesn’t forbid anything. That makes it easy for people to stick with it for a long time, she said.
Hu added that the diet’s flexibility makes it adaptable to many cuisines.
“As an example, an Asian individual might use tofu as a protein source and replace white rice with brown rice,” he said. “Individuals can incorporate traditional recipes from other cultures and locally available foods while maintaining the MedDiet‘s key principles.”

Book Review
Invisible Labor: The Untold Story of the Cesarean Section
By Rachel Somerstein
Ecco: 336 pages, $32
If you buy books linked on our site, The Times may earn a commission from Bookshop.org, whose fees support independent bookstores.
After Rachel Somerstein was rushed into an operating room for an unplanned caesarean section, her doctor made the first cut. “I felt that,” she told him. “You’ll feel pressure,” the doctor responded.
But, horrifyingly, Somerstein “felt it all: the separation of my rectus muscles; the scissors used to move my bladder; the scalpel, with which he ‘incised’ my uterus.” When her daughter was born, Somerstein was so traumatized that she couldn’t hold her baby. She screamed for her to be taken from the room.
Friends encouraged Somerstein to file a lawsuit; others balked, doubting that she could have undergone major abdominal surgery without anesthesia. The overarching message to mothers who experience traumatic delivery in this country is to get over it. “How long did it really take,” one attorney asked the author, “five minutes?”
It’s a common refrain: Just be happy you have a healthy baby. The dangerous and potentially unnecessary interventions of medicalized childbirth are never called into question when the pain and trauma of the person giving birth are invalidated. Somerstein quotes two scholars of healthcare and science: “Something is visible [only] when somebody recognizes it as relevant.”
Propelled by Somerstein’s own experience, “Invisible Labor” is a thorough investigation of birthing practices grounded in misogyny, racism and other forces contrary to the well-being of mothers.
Somerstein illuminates the capitalistic drive to rush birth in American hospitals facing infrastructural and staffing deficiencies: “Compared with vaginal births, C-sections are more efficient. Particularly if they are scheduled, a hospital can do far more of them … in a day.”
The medicalization of childbirth, including the C-section, undoubtedly saves lives. But the dehumanization of those giving birth, and the erasure of their well-being and experience, hurts everyone. As “Invisible Labor” shows, the lack of attention and communication in the hospital setting can be fatal.
Somerstein delves into the history of the C-section, which was devised to help save both mother and child. It was quickly adapted by enslavers, however, in “a push to bring about more slaves. In the U.S., most early caesareans took place in the South, and they still do today; a disproportionate number of Black and enslaved women made up the subjects.”
The history of birthing in the U.S. becomes a means of grappling with the history of slavery, racism and eugenics. Once the C-section was in practice, doctors realized that they could also sterilize women of color and those deemed disabled without their consent. “ ‘Acabó la canción,’ said one woman sterilized at L.A. County Hospital in the 1970s. My song has ended.”
Rachel Somerstein
(Joe Lingeman)
Relying on essential feminist texts such as Adrienne Rich’s “Of Woman Born: Motherhood as Experience and Institution,” Somerstein amplifies the role of the midwife — and her removal from the delivery room, taking away a library’s worth of knowledge about birth and birthing people and placing them in largely inexperienced, male hands.
“Just as land gets colonized, so does knowledge,” Barbara Katz Rothman, a sociologist, told Somerstein. “By laying claim to birth, medicine established boundaries over who has authority to attend it.”
Shockingly, Somerstein’s research shows that the electronic fetal monitoring technology used in hospitals, known as EFM, is “notoriously unreliable.” Often, it reports a falling fetal heart rate or stalled labor when the baby and mother are perfectly healthy. But it allows doctors and nurses to tend to many patients, running from room to room and leaving patients alone. Doctors and nurses are trained in the technology instead of the skills of midwives, who know what to look for from extensive experience.
“When used on mothers who have not previously had a caesarean,” Somerstein writes, “EFM, according to one study, makes a person up to 81 percent more likely to have a C-section than mothers monitored intermittently.”

The C-section rate has grown and grown — to about 1 in 3 U.S. births — and “a C-section mom is about 80 percent more likely to have a serious complication, like needing a blood transfusion or an emergency hysterectomy.” Women of color and particularly Black women are more likely to have caesareans.
Speaking to Rei Shimizu, a social work researcher, Somerstein relates: “There’s an assumption in the health system … that nonwhite female bodies cannot give birth safely without intervention.”
“Obstetric racism is about white doctors being racist, but it’s also about doctors, white, Black, whatever, that when you’re expressing your concerns, they just don’t listen,” said Nicole Carr, a professor who spoke to Somerstein about losing her baby after her concerns about her pregnancy were ignored. “It’s a system that makes it so that when you go in and talk about your concerns, it’s almost like you’re not an expert in your own body.”
“Invisible Labor” does not claim that doctors or even medicalized childbirth is the problem. Rather, it’s a system that decenters our humanity and relies on technology and statistics.
“We believe this visual omniscience will fix the problem,” Somerstein writes. “And we discard or forget that events take place outside the frame, including what subjective, embodied knowledge can reveal.”
Women who experience traumatic childbirth are far more likely to suffer from postpartum depression, anxiety or both. Perhaps “attending to women’s pain could be rectified by the simple but radical decision to ask women how they feel and listen to the answer,” Somerstein writes. Instead of telling her “You’ll feel pressure” when he made the incision, her doctor could have asked, “Do you feel pressure?” or, even better, “Do you feel pain?”
Then again, what do we expect in a country whose Supreme Court struck down women’s bodily autonomy? As it stands now, an unborn fetus has more rights than a woman or girl in many states. To create a better system of childbirth for mothers, we have to believe that the rights and indeed the lives of pregnant people matter.
“Invisible Labor” clearly and compassionately blends scientific research and reportage with the personal stories of Somerstein and other women. Childbirth is painful, but with the right care, it can also ground us in our humanity.
Some of the most moving accounts of birth in “Invisible Labor” come from women who had the support of a doula or midwife. When Somerstein writes that “every woman deserves the touch of a midwife,” she is communicating that every person deserves someone who will listen to and validate their experience. This should be the first standard of care.
Jessica Ferri is the owner of Womb House Books and the author, most recently, of “Silent Cities San Francisco.”

Los Angeles could soon end its requirement for city employees to be vaccinated against COVID-19.
City officials are recommending that the Los Angeles City Council halt the requirement as soon as early June, according to a newly released report. The COVID vaccination rule was first approved by city leaders nearly three years ago as public health officials urged vaccination to protect people from the coronavirus.
In a report, City Administrative Officer Matt Szabo noted that other local government agencies — including the cities of Long Beach and San Diego and Los Angeles County — had stopped requiring COVID vaccination as a condition of employment. Szabo said L.A. employee groups had not opposed ending the requirement.
The L.A. ordinance defined “fully vaccinated” as workers having received either one dose of a single shot vaccine, such as the Johnson & Johnson shot, or both doses of a vaccine that required two shots, such as the Moderna or Pfizer vaccines, but said the definition “may be expanded” if health officials required boosters. Under the city ordinance, workers could seek an exemption if they had “a medical condition or restriction or sincerely held religious beliefs.”
If city leaders approve ending the requirements, employees who resigned or were terminated because of the vaccination rule may be eligible to be rehired in the same positions as before.
Eighty-six city workers were terminated under the rule, Szabo said; it is unclear how many employees resigned over the COVID vaccination requirement because they do not have to report their reasons.
Los Angeles has faced numerous lawsuits over its COVID vaccination rule. In one of the latest suits, filed last week in federal court, a woman formerly employed as a city accountant said she was denied a religious exemption from the vaccination requirement and ultimately discharged from her position. She accused the city of discrimination, saying it had ignored its policy of “accommodating sincerely held religious beliefs.”
The move to halt the vaccination requirements comes as the Los Angeles County Department of Public Health has seen a slight uptick in COVID cases, although they cautioned that it was too soon to say if it would become a sustained increase.

Sioux Falls Eatery Earns 'Best Burrito in South Dakota' Honor
Tennessee baseball powers through Indiana and advances to Regional Final

Pope Francis calls Texas AG Ken Paxton’s attacks on El Paso’s Annunciation House ‘madness’

Utah National Guard’s State Partnership Program brings healthcare to underserved Moroccan people

Longtime Vermont Sen. Dick Sears dies at 81

See it: Tesla crashes into Columbus convention center at 70 mph

Colorado Rockies game no. 116 thread: Zac Gallen vs José Ureña

Fox News Politics: Georgia the whole day through

Death of missing Oregon girl found in stream ruled homicide

At least 2 dead as tornadoes hit Alabama, damage homes across Southeast

Trump joins TikTok, the app he once tried to ban as president

Businesswoman Halla Tomasdottir set to become Iceland’s next president

Vintage Trump remarks after convictions renew dilemma for news media and voters alike

Ron DeSantis touts Florida's education system, slams 'woke' academia in Sarasota address

Thousands march in Budapest streets in support of Orbán
-
 News1 week ago
News1 week agoRead the I.C.J. Ruling on Israel’s Rafah Offensive
-
 News1 week ago
News1 week agoVideo: Protesters Take Over U.C.L.A. Building
-
 World1 week ago
World1 week agoHoping to pave pathway to peace, Norway to recognise Palestinian statehood
-
 News1 week ago
News1 week agoLegendary U.S. World War II submarine located 3,000 feet underwater off the Philippines
-
 World1 week ago
World1 week agoFamilies of Uvalde school shooting victims sue Microsoft, Meta and gunmaker
-
 Politics1 week ago
Politics1 week agoHunter Biden attends pre-trial hearing in Delaware court on federal gun charges
-
 Politics1 week ago
Politics1 week agoDefense Secretary Lloyd Austin to undergo nonsurgical procedure, Deputy Kathleen Hicks will assume control
-
 News1 week ago
News1 week agoHere are three possible outcomes in the Trump hush money trial : Consider This from NPR