Science
Fed up with perimenopause or menopause? The We Do Not Care Club is here for you

Melani Sanders is over it.
She’s over meticulously applying makeup before leaving the house or, even, having to wear a bra when running errands. She’s over wasting time plucking chin hairs, searching for brain fog-induced lost reading glasses and — most of all — withholding her opinions so as not to offend others.
As a 45-year-old perimenopausal woman, Sanders is no longer searching for outside validation and is over people-pleasing.
The dedication page in her new book sums it up best: “To the a— who told me I had a “computer box booty.”
Who is this dude, and is Sanders worried about offending him?
She doesn’t care.
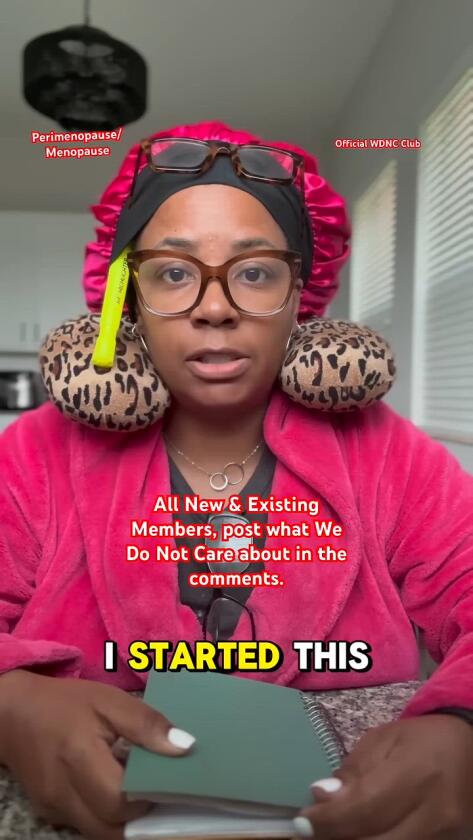
Author, Melani Sanders, in an outfit she typically wears in her social media videos.
(Surej Kalathil Sunman Media)
That’s Sanders’ mantra in life right now. Last year, the West Palm Beach, Fla.-based mother of three founded the We Do Not Care Club, an online “sisterhood” into the millions of perimenopausal, menopausal and post-menopausal women “who are putting the world on notice that we simply do not care much anymore.” Sanders’ social media videos feature her looking disheveled — in a bathrobe and reading glasses, for example, with additional pairs of reading glasses hanging from her lapels — while rattling off members’ comments about what they do not care about anymore.
“We do not care if we still wear skinny jeans — they stretch and they’re comfortable,” she reads, deadpan. “We do not care if the towels don’t match in our house — you got a rag and you got a towel, use it accordingly.”
Sanders’ online community of fed up women grew rapidly. She announced the club in May 2025, and it has more than 3 million members internationally; celebrity supporters include Ashley Judd, Sharon Stone and Halle Berry. It’s a welcoming, if unexpected, space where women “can finally exhale,” as Sanders puts it. The rallying cry? “We do not give a f—ing s— what anyone thinks of us anymore.”
That’s also the message of Sanders’ new book, “The Official We Do Not Care Club Handbook: A Hot-Mess Guide for Women in Perimenopause, Menopause, and Beyond Who Are Over It.” The book is part self-help book, with facts about the perimenopause and menopause transition; part memoir; part practical workbook with tools and resources; and part humor book, brimming with Sanders’ raw and authentic comedic style. (It includes a membership card for new club inductees and cutout-able patches with slogans like “lubricated and horny” or “speaking your truth.”)
We caught up with Sanders while she was in New York to promote her book and admittedly “overstimulated from all the horns,” she said. But she just. Did. Not. Care.
This interview has been edited for length and clarity.
The We Do Not Care Club came about after you had a meltdown in a supermarket parking lot. Tell us about that.
I was in the parking lot of Whole Foods. I needed Ashwagandha — that was my holy grail at the time for my perimenopause journey, and I was out of it. I got back in my car and looked at myself in the rear view mirror. I had on a sports bra that was shifted to one side. My hair was extremely unstructured. I had a hat on and socks mismatched — I was a real hot mess. Nothing added up. But in that moment, I realized that I just didn’t care much anymore. I just said, “Melanie, you have to take the pressure off, girlfriend. It’s time to stop caring so much.” I decided to press the record button and see if anyone wanted to join me in starting a club called the We Do Not Care Club. I released the video and drove home, which took about 20 minutes, and by the time I got home it had [gone viral].
You got hundreds of thousands of new followers, internationally, within 24 hours. Why do you think the post resonated so greatly at that moment?
I had to dissect that because it was kind of unreal. Like, what is it about country, old Melanie that hit record and asked about a little club that she thought maybe 20 or 30 women would want to join? Over the summer, I studied this and did more videos and I listened. It was the relatability. It was the understanding. It was just letting my guard down and just saying it out loud. Speaking my truth. Also, for many women, we have this silent pressure to get it all done. But we’re at capacity. In the book, I talk about how, once I was in perimenopause, I didn’t want to have sex with my husband. I didn’t want to see my kids — like, everyone just close the door! And that’s kind of shameful, you know? It’s not like I don’t love my family. I really do. But I can’t do it all anymore. And I just think that resonated with a lot of sisters throughout the world. It was like: Now is the time for us to just explode and I think we all did it at once.
“The Official We Do Not Care Club Handbook.”
(William Morrow)
You entered perimenopause (or “Miss Peri,” as you call it) at age 44, after a partial hysterectomy. How did your life change after that?
I did not expect it. I knew that I had fibroids and I was uncomfortable because of that. So when I had the hysterectomy, I was expecting to now be a whole person again afterwards. But I just went into this dark place. It was like you’re fighting against yourself to just be normal again. And your body is changing in so many ways. For me, that was the hot flashes, the insomnia, the depression, the rage. My joints were really, really stiff all of a sudden. It’s like, ‘wait a minute, how and why?!!’ And [I got] frozen shoulder. Frozen shoulder was how I discovered I was in perimenopause because I was not told by my doctor who performed my hysterectomy that this could happen. And I didn’t know where to turn or where to go because I was just being told everything was normal. I was so frustrated with the process, the lack of education, the lack of resources. The lack of compassion, I would even say.
Your book and social media videos are so funny. Do you have a comedy background?
I don’t, and I get asked that often. I just say what’s on my mind and sometimes, I guess, it comes out funny — but I’m not trying. The [wearing multiple pairs of] glasses: I do that because, with perimenopause, my eyesight went bad really quickly. I was out in public one day and I could not read. I was just traumatized. So every time I would see glasses, I would just put them on me because I don’t want to get stuck without them. That neck pillow, when I got frozen shoulder, I was using it a lot. Then one day when I hit record, I had the neck pillow on and I just didn’t care. And it stuck.
You’ve appeared on TV, been featured in publications, and People magazine named you creator of the year for 2025. What has this sudden fame been like for you?
It’s surreal. I have not completely processed it yet. It’s a lot to take in. I’m just an everyday woman that decided to press record and accidentally started a movement. Impostor syndrome is there from time to time. But I’m just trying my best to accept everything that’s going on — and keep just being Melani.

Has the overwhelming response from new members fueled your own resolve to be true to yourself or otherwise changed you personally?
It absolutely has. It’s the strength that the sisterhood gives me. Because I’m very scared. You know, the book is coming out. And the tour is sold out in several cities. This is all within an eight-month span. It’s a lot. But when everyone is saying they love you, and when you have a group of women that understands you and feels the way that you feel, absolutely, there’s strength in numbers. Now I don’t care about making mistakes.
You live in a very male household. What do your sons and husband think of all this?
Once I decided that I didn’t care anymore, I just expected for them to kind of allow things just to go to hell around the house — but it was quite the opposite. All three of my sons and my husband, they’re just very supportive. Because it was very sad for me. It was very hard to not want to watch movies or anything and just be by myself. But they rose to the occasion and they make sure things are done when they’re home. They really show how they love their mom during this time.
How can other men become allies to the women they love during the menopause transition?
Just either get out of our way or, you know, just kind of read the room! Because we don’t know who we are from day to day. We don’t know what’s gonna ache. We don’t know what’s going to hurt or what’s going to itch or what’s going to be dry. And if it’s an off day, then darling, it’s just an off day — and it’s OK.
What are some things that you do still care about greatly?
I care about sisterhood. Because when women bind together, it’s a game changer. We will move mountains. I just think that, in this world, there’s so much pressure, so much overstimulation. So I care about being able to live authentically. To feel free. To be OK with who you are. Within WDNC, the two things that I definitely want to convey that I care about is: that you are enough. And you are not alone. And of course I love my kids. I love my family immensely.

Where does the WDNC go from here? What’s the future?
Retreats. That is definitely a dream. To have a weekend retreat where women can come and the only thing that you need to bring is some clean underwear and some pantyliners! (You can’t have a good, hard laugh or a good sneeze or a good cough without pissing your pants.) No makeup, no nothing, just come and be free. I want three different rooms. One will be the rage room and you’ll go in there and just throw stuff around and scream and punch, whatever you want. Then a quiet room. No talking, no nothing, just silence. And the last room will be the “Let that s— go room.” That’s where we’ll put everything that we have in us, that we’re holding onto that’s keeping us from living a blissful and peaceful life, and write it down and let it go. I just want to touch sisters and let them know it is OK. We are OK. I have my s— I go through. You have your s— you go through. It’s OK. Let’s live.

new video loaded: NASA Announces Artemis III Crew
transcript
transcript
NASA Announces Artemis III Crew
NASA announced the crew of Artemis III mission, which will fly to low-Earth orbit to test rendezvous and docking maneuvers with one or two lunar landers.
-
“I am excited to welcome you as the next crew in the Artemis journey to successfully return to the moon — this time to stay.” “I’m honored by the role that I’ve been given. I’m also very humbled by the task in front of us. But first and foremost, I’m grateful.” “So with that, the Artemis II crew, comrade, hands you the baton. You got the controls.” “As you know, we had a significant anomaly at our Launch Complex 36A on May 28. We’ve redoubled our efforts and are moving forward.”
By Alisa Shodiyev Kaff
June 9, 2026
Science
Santa Monica Mountains’ last steelhead trout survived the Palisades fire — and even had babies

Scientists feared the Santa Monica Mountains’ last remaining steelhead trout were dead, smothered by debris flows unleashed by the Palisades fire.
But the endangered fish surprised them: A team of biologists recently spotted 30 of the rare trout — and 21 babies — in Topanga Creek.
“There was a lot of happy dancing in the creek,” said Rosi Dagit, principal conservation biologist for the Resource Conservation District of the Santa Monica Mountains, which works with public and private landowners to conserve natural resources.
That’s because the steelhead here are endangered, at both the state and federal levels. Once, they swam in most streams of the Santa Monicas, but their numbers plummeted amid overfishing and coastal development. Increasingly frequent wildfire has further stressed their habitat. Topanga Creek, a biodiversity hot spot, is home to their last known population in the mountains that stretch from the Hollywood Hills to Point Mugu in Ventura County.
The trout that were spotted, including this one, are part of a distinct Southern California population that’s listed as endangered at the state and federal levels.
(RCDSMM Stream Team)
The California Department of Fish and Wildlife spearheaded a complex mission to rescue trout threatened by the Palisades fire that sparked in January 2025.
Time was of the essence. The fire hadn’t yet been fully contained. But rain was on the way, which would sweep massive amounts of sediment from the denuded hillsides into the water. Fish are often killed this way.
Crews stunned the fish with electricity, scooped them up in buckets, trucked them to a hatchery and ultimately moved them to Arroyo Hondo Creek in Santa Barbara County.
Within days, Topanga Creek was choked with mud. Some assumed the fish left behind were goners.
But in March, the conservation district’s team found four. The following month, when water conditions were clearer, they saw more.
“These fish continue to amaze me,” said Kyle Evans, environmental program manager for the state Department of Fish and Wildlife, who had seen the damage to the creek. “I had seen populations get wiped out in similar situations. So when I heard, I was thrilled.”
Evans surmises the fish that survived were in an area of the creek where less charred material and sediment were swept in.
“These fish likely hunkered down, were hiding under some rocks or places to try to get away from the main concentration of flow,” he said. “And luckily they weren’t buried.”
The ones that were spotted were fairly small, around 6 to 14 inches. Rainbow trout and steelhead trout are the same species, but with different lifestyles. If the fish remain in freshwater, they’ll be considered rainbows. However, they can migrate to the ocean and become steelhead, where they typically grow larger before returning to their natal waters to spawn.
Topanga Creek hasn’t fully recovered from the damage it sustained, but scientists say it’s looking better. Surveys last year were “so depressing,” Dagit said, with very few animals, and stretches that were essentially transformed into flat roads from all the sediment buildup. Some of the riparian canopy burned right down to the creek.
Then came 32 inches of rain over the last nine months, scouring out and moving sediment, creating deeper pools. Dagit said they recently found newt egg masses for the first time in years, as well as a few adult newts and many frogs. Plants that provide cover are starting to recover.
She provided photos comparing certain pools last year and this year, some dramatically transformed. In September 2025, the Shrine Pool could have been an overgrown hiking trail. This April, it was filled with shallow water.

The Shrine Pool in September 2025, left, and the same location in April 2026, right, with RCDSMM’s Isaac Yelchin donning a wetsuit.
(RCDSMM Stream Team)
Topanga Creek is home to another endangered fish, the small but hardy northern tidewater goby, often described as cute. Not long before the trout operation, Dagit led a rescue of hundreds of these fish too. Many were repatriated to the lagoon at the mouth of the creek in a moving ceremony last June.
There’s still the matter of what to do with the trout that were moved to Santa Barbara County last year. Evans would like to bring them home to the Santa Monicas at some point, but isn’t sure if it will happen. On one hand, they could bolster the small, genetically isolated surviving population. On the other, they might inadvertently bring in a disease or bacteria. There is some time to decide. Evans estimates the creek still needs to recover for two to three more years.
For now, the fish are functioning fine in their adopted creek. Experts worried the trauma wrought by the move would disrupt their spawning process, but they had babies that spring. This year, they spawned again.

The Pacifica Municipal Pier was shut down and taped off Thursday after city workers noticed cracks running through the landmark structure and concrete chunks falling into the ocean.
It’s just one of many coastal California structures that have recently crumbled under pressure from a rising and relentless ocean.
Officials from the small, beach city south of San Francisco said the pier was closed due to “cracking, separation, and displacement of the concrete walkway and structural elements.”
It will stay closed while structural engineers asses its safety.
Photos taken by city employees show a wide crack that runs from top to bottom and across the structure as well. Other photos show a large horizontal crack under the foundation of a small restaurant on the pier, the Chit Chat Cafe.
The cafe was also shut down.
This is not the first time the 53-year-old pier has shown signs of stress. In 2021, part of it was shut down after handrails along the edge collapsed. And in 2023, after a series of storms pummeled the Central California coast, damaging parts of the pier, the structure was partially closed for more than year.
Those same storms caused extensive damage in Aptos and Capitola, 70 miles south, where piers and waterfront infrastructure were swept away or damaged.
In 2024, a 150- to 180- foot section of the Santa Cruz wharf was ripped off by powerful waves.
At least 10 of the state’s dozens of coastal public piers were closed for part or all of 2024 due to structural damage sustained in winter storms since 2022. At least five others have longer-term upgrades planned to address structural issues.
“These things are costly to maintain,” said Zach Plopper, senior environmental director at Surfrider. “They are a part of our California coastal culture in many ways, but we’re going to need to reckon with, one, the state that they’re in, and two, the continuous and worsening threats they’re going to experience,”
He said most of the piers were constructed in the early 1900s, and they weren’t built to withstand decades of rough seas, storms and rising sea level.
“With this incoming El Niño, which is forecasted to be significant, and this marine heat wave we’re in the midst of, we’re kind of in uncharted waters as far as what this winter could bring in terms of storms and swells to the California coast, and we’re likely going to see a lot more damage,” he said. “Not just piers, but roads and other coastal infrastructure up and down the state.”
There was no storm in Pacifica earlier this week, so no single event could be blamed for the destruction.
However, a 2025 report from an outside engineering firm, GHD, found that several sections of the pier were in “poor” or “serious” condition, and they recommended closure before anticipated storms or events that could “subject the piles to high winds, swells and large waves.”
The firm found several areas of the pier where concrete was missing and rebar was exposed and corroding.
“The pier has continued to experience high winds and large waves in a harsh marine environment,” the engineers wrote in the report, noting that continuous exposure to seawater or marine spray was “detrimental” to the structure.
A 2023 city report estimated it would cost $19 million to repair.
That same year, a state law was enacted to require local governments along the California coast to plan for sea level rise in the coming decades.
Sea level has risen some 8 inches, on average, along the coast in the past 150 years, Plopper said, and researchers anticipate another foot in the next 25 years.
“We’re going to see profound shifts on our coastline, none that we have ever experienced before, and building static structures on the coast just doesn’t work all that well,” he said. “We’re going to have to make some really hard decisions.”
-

 South Dakota5 minutes ago
South Dakota5 minutes agoWhat to know about the SD’s first gubernatorial runoff
-

 Tennessee12 minutes ago
Tennessee12 minutes agoComparing Tennessee’s Neyland Entertainment District to others in college sports
-

 Texas15 minutes ago
Texas15 minutes agoWhere to watch Texas Rangers vs Kansas City Royals: TV channel, start time, streaming for June 10
-

 Utah20 minutes ago
Utah20 minutes agoNew NBA Draft Intel: AJ Dybantsa, Darryn Peterson and Utah
-

 Vermont27 minutes ago
Vermont27 minutes agoVermont Green FC plays Canada’s national soccer team in World Cup tuneup – VTDigger
-

 Virginia30 minutes ago
Virginia30 minutes agoNavy sailor sentenced to 44 years for killing fellow service member Angelina Resendiz in his Virginia barracks room
-
Washington35 minutes ago
Where to watch Washington Nationals vs San Francisco Giants: TV channel, start time, streaming for June 10
-

 Wisconsin42 minutes ago
Wisconsin42 minutes agoChris Borland heads back to Wisconsin as Hall of Fame inductee

