Science
Mounjaro bests Ozempic for weight loss in first head-to-head comparison of real-world use

In the first head-to-head comparison of two blockbuster drugs used in real-world conditions, people who took Mounjaro lost significantly more weight than their counterparts who took Ozempic — and the longer the patients kept taking the drugs, the wider the gap became.
After three months of weekly injections, patients on Ozempic lost 3.6% of their body weight, on average, while those on Mounjaro lost an average of 5.9%.
At the six-month mark, Ozempic patients had dropped an average of 5.8% of their weight, while the average weight loss for Mounjaro patients was 10.1%.
And when a full year had passed, those taking Ozempic had lost an average of 8.3% of their weight, while those taking Mounjaro had shed an average of 15.3%.
The researchers who conducted the analysis also found that compared with people on Ozempic, those on Mounjaro were 2.5 times more likely to lose at least 10% of their initial weight and more than three times as likely to lose at least 15% of their weight during their first year on the medications.
The findings were published Monday in JAMA Internal Medicine.
Dr. Matthew Freeby, an endocrinologist and director of the Gonda Diabetes Center at UCLA’s Geffen School of Medicine, said the study results are in line with what he has observed in his own patients.
“From a weight-loss perspective, and from a sugar-lowering perspective for those with Type 2 diabetes, we see stronger effects with Mounjaro compared to Ozempic,” said Freeby, who was not involved in the research.
Both drugs were approved by the U.S. Food and Drug Administration to help people with diabetes keep their blood sugar under control. By mimicking a hormone called glucagon-like peptide 1, or GLP-1, they boost the body’s production of insulin, slow digestion, increase feelings of satiety and reduce appetite.
Mounjaro also imitates a related hormone called glucose-dependent insulinotropic peptide, or GIP.
When the drugs were tested against placebos in clinical trials, both helped patients lose a significant amount of weight. Tirzepatide, the active ingredient in Mounjaro, appeared to be more effective than semaglutide, the active ingredient in Ozempic. But the trials weren’t conducted under the same conditions, so the results aren’t directly comparable.
Researchers from Truveta, a healthcare data and analytics company owned by 30 health systems, sought to remedy that by examining their trove of electronic health records. The work also gave them a chance to see how patients fared outside the idealized setting of a clinical trial, which typically provides free medication, regular check-ups and other types of support.
With the help of their database, the researchers were able to spot people who filled their first prescription for either drug between May 2022 — the month Mounjaro joined Ozempic in receiving FDA approval — and September 2023. Patients didn’t need to have Type 2 diabetes to be included in the study, but they did have to be overweight (with a body mass index of at least 27) or obese (with a BMI of at least 30).
The Truveta team found about 41,000 people across more than 30 states who met all their criteria for being included in the study. Since Ozempic patients outnumbered Mounjaro patients by a margin of 3-to-1, the researchers used information on age, race, income, health history and other factors to come up with a group of Ozempic patients that most closely matched the Mounjaro patients. The result was a population of nearly 18,400 who were evenly split between the two drugs.
Before their first medication dose, the average weight for people in both groups was 243 pounds. But it didn’t take long for the two groups to diverge.
After accounting for unmeasured influences that could have skewed the results, the Truveta team found that the amount of weight lost was 2.4 percentage points higher for Mounjaro patients than for Ozempic patients after three months, 4.3 percentage points higher after six months, and 6.9 percentage points higher after a year.
Mounjaro also bested Ozempic in terms of people’s success in meting various milestones within a year of starting on one of the drugs.
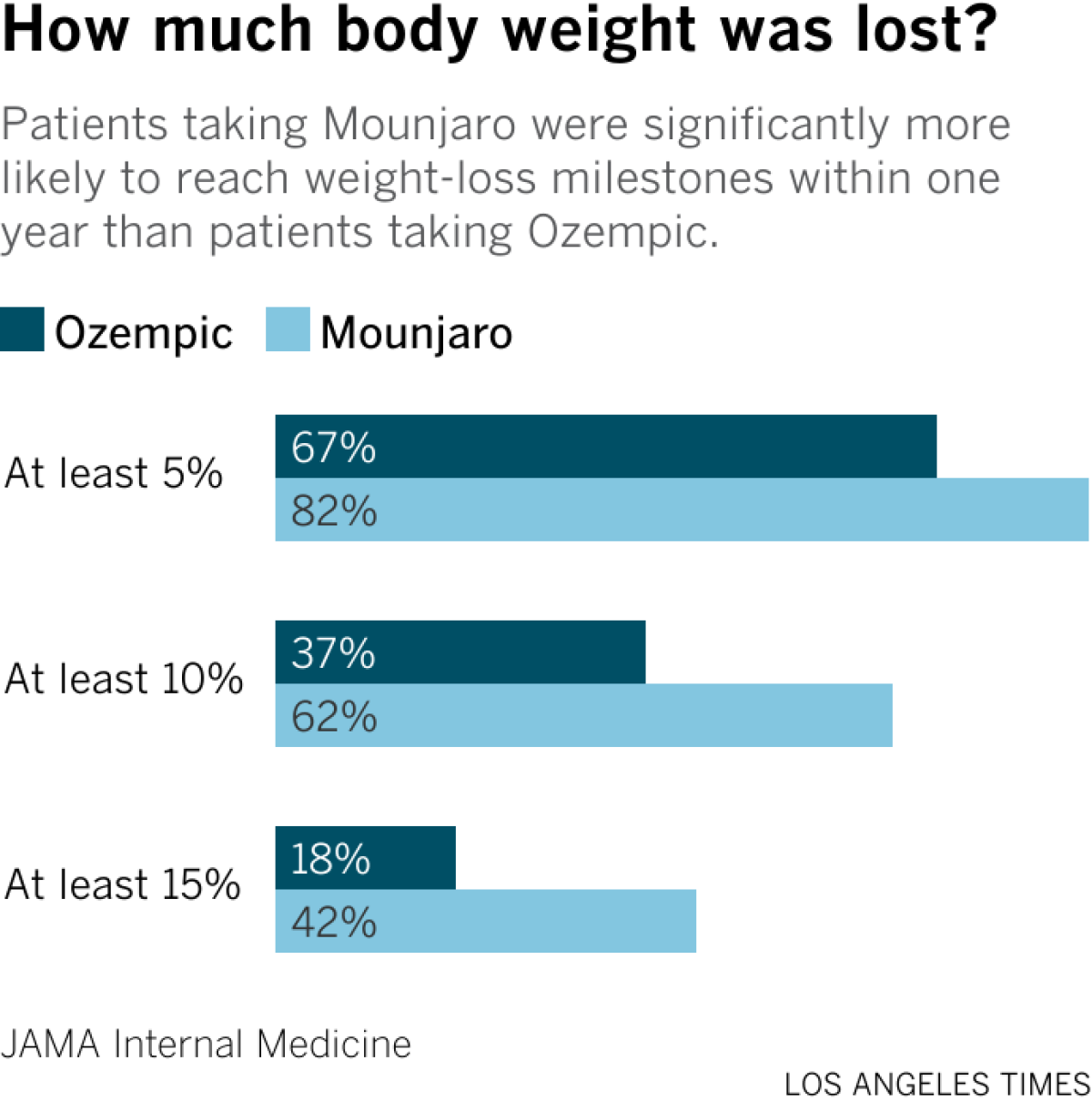
Nearly 82% of Mounjaro patients lost at least 5% of their body weight, compared with 67% of patients who took Ozempic. Likewise, 62% of Mounjaro patients and 37% of Ozempic patients lost at least 10% of their initial weight, while 42% of Mounjaro patients and 18% of Ozempic patients lost at least 15% of their starting weight.
The researchers didn’t examine the biological mechanisms of the two drugs, but study leader Tricia Rodriguez, a principal applied scientist with Truveta Research, said Mounjaro may have been more effective because it works two ways instead of just one.
The big gap in effectiveness wasn’t accompanied by a measurable difference in the rate of moderate or severe side effects like bowel obstructions and pancreatitis, which were rare for patients in both groups. The researchers didn’t compare the risk of milder problems like nausea and vomiting because people wouldn’t necessarily report them to their doctors, Rodriguez said.
Regardless of which drug they took, patients with Type 2 diabetes lost less weight than patients without the disease, the researchers found. That might be explained by the fact that certain diabetes treatments can cause weight gain, and that some patients eat more throughout the day to keep their blood sugar from getting too low, Freeby said.
It’s also possible that people who sought prescriptions for Ozempic or Mounjaro with the goal of slimming down were more motivated to keep taking the drug even if it was expensive or caused uncomfortable side effects, or that they were more likely to adopt other behaviors that promote weight loss, Rodriguez said.
Figuring this out is “a crucial topic for future research,” she said.
People currently taking Ozempic likely have a more pressing question on their minds: Should I switch to Mounjaro?
Dr. Nick Stucky, an infectious disease physician at Providence Portland Medical Center and the study’s senior author, said the results alone should not cause patients to stop taking a drug that is working for them. The risk of side effects, insurance coverage and drug availability are things to consider as well.
“While tirzepatide was significantly more effective than semaglutide, patients on both medications experienced substantial weight loss,” said Stucky, who is also Truveta’s vice president of research.
Freeby seconded that opinion.
“If someone is doing well with a medication, why rock the boat?” he said.
Freeby added that Ozempic (and its sister medication Wegovy, which is FDA-approved specifically for weight loss) has at least one advantage over Mounjaro (and Zepbound, its weight-loss counterpart): In clinical trials, Ozempic has been shown to reduce the risk of heart attacks, strokes and other cardiovascular problems as well as kidney failure.
“At this point, we don’t have a lot of data on Mounjaro when it comes to secondary outcomes,” he said.

new video loaded: NASA Announces Artemis III Crew
transcript
transcript
NASA Announces Artemis III Crew
NASA announced the crew of Artemis III mission, which will fly to low-Earth orbit to test rendezvous and docking maneuvers with one or two lunar landers.
-
“I am excited to welcome you as the next crew in the Artemis journey to successfully return to the moon — this time to stay.” “I’m honored by the role that I’ve been given. I’m also very humbled by the task in front of us. But first and foremost, I’m grateful.” “So with that, the Artemis II crew, comrade, hands you the baton. You got the controls.” “As you know, we had a significant anomaly at our Launch Complex 36A on May 28. We’ve redoubled our efforts and are moving forward.”
By Alisa Shodiyev Kaff
June 9, 2026
Science
Santa Monica Mountains’ last steelhead trout survived the Palisades fire — and even had babies

Scientists feared the Santa Monica Mountains’ last remaining steelhead trout were dead, smothered by debris flows unleashed by the Palisades fire.
But the endangered fish surprised them: A team of biologists recently spotted 30 of the rare trout — and 21 babies — in Topanga Creek.
“There was a lot of happy dancing in the creek,” said Rosi Dagit, principal conservation biologist for the Resource Conservation District of the Santa Monica Mountains, which works with public and private landowners to conserve natural resources.
That’s because the steelhead here are endangered, at both the state and federal levels. Once, they swam in most streams of the Santa Monicas, but their numbers plummeted amid overfishing and coastal development. Increasingly frequent wildfire has further stressed their habitat. Topanga Creek, a biodiversity hot spot, is home to their last known population in the mountains that stretch from the Hollywood Hills to Point Mugu in Ventura County.
The trout that were spotted, including this one, are part of a distinct Southern California population that’s listed as endangered at the state and federal levels.
(RCDSMM Stream Team)
The California Department of Fish and Wildlife spearheaded a complex mission to rescue trout threatened by the Palisades fire that sparked in January 2025.
Time was of the essence. The fire hadn’t yet been fully contained. But rain was on the way, which would sweep massive amounts of sediment from the denuded hillsides into the water. Fish are often killed this way.
Crews stunned the fish with electricity, scooped them up in buckets, trucked them to a hatchery and ultimately moved them to Arroyo Hondo Creek in Santa Barbara County.
Within days, Topanga Creek was choked with mud. Some assumed the fish left behind were goners.
But in March, the conservation district’s team found four. The following month, when water conditions were clearer, they saw more.
“These fish continue to amaze me,” said Kyle Evans, environmental program manager for the state Department of Fish and Wildlife, who had seen the damage to the creek. “I had seen populations get wiped out in similar situations. So when I heard, I was thrilled.”
Evans surmises the fish that survived were in an area of the creek where less charred material and sediment were swept in.
“These fish likely hunkered down, were hiding under some rocks or places to try to get away from the main concentration of flow,” he said. “And luckily they weren’t buried.”
The ones that were spotted were fairly small, around 6 to 14 inches. Rainbow trout and steelhead trout are the same species, but with different lifestyles. If the fish remain in freshwater, they’ll be considered rainbows. However, they can migrate to the ocean and become steelhead, where they typically grow larger before returning to their natal waters to spawn.
Topanga Creek hasn’t fully recovered from the damage it sustained, but scientists say it’s looking better. Surveys last year were “so depressing,” Dagit said, with very few animals, and stretches that were essentially transformed into flat roads from all the sediment buildup. Some of the riparian canopy burned right down to the creek.
Then came 32 inches of rain over the last nine months, scouring out and moving sediment, creating deeper pools. Dagit said they recently found newt egg masses for the first time in years, as well as a few adult newts and many frogs. Plants that provide cover are starting to recover.
She provided photos comparing certain pools last year and this year, some dramatically transformed. In September 2025, the Shrine Pool could have been an overgrown hiking trail. This April, it was filled with shallow water.

The Shrine Pool in September 2025, left, and the same location in April 2026, right, with RCDSMM’s Isaac Yelchin donning a wetsuit.
(RCDSMM Stream Team)
Topanga Creek is home to another endangered fish, the small but hardy northern tidewater goby, often described as cute. Not long before the trout operation, Dagit led a rescue of hundreds of these fish too. Many were repatriated to the lagoon at the mouth of the creek in a moving ceremony last June.
There’s still the matter of what to do with the trout that were moved to Santa Barbara County last year. Evans would like to bring them home to the Santa Monicas at some point, but isn’t sure if it will happen. On one hand, they could bolster the small, genetically isolated surviving population. On the other, they might inadvertently bring in a disease or bacteria. There is some time to decide. Evans estimates the creek still needs to recover for two to three more years.
For now, the fish are functioning fine in their adopted creek. Experts worried the trauma wrought by the move would disrupt their spawning process, but they had babies that spring. This year, they spawned again.

The Pacifica Municipal Pier was shut down and taped off Thursday after city workers noticed cracks running through the landmark structure and concrete chunks falling into the ocean.
It’s just one of many coastal California structures that have recently crumbled under pressure from a rising and relentless ocean.
Officials from the small, beach city south of San Francisco said the pier was closed due to “cracking, separation, and displacement of the concrete walkway and structural elements.”
It will stay closed while structural engineers asses its safety.
Photos taken by city employees show a wide crack that runs from top to bottom and across the structure as well. Other photos show a large horizontal crack under the foundation of a small restaurant on the pier, the Chit Chat Cafe.
The cafe was also shut down.
This is not the first time the 53-year-old pier has shown signs of stress. In 2021, part of it was shut down after handrails along the edge collapsed. And in 2023, after a series of storms pummeled the Central California coast, damaging parts of the pier, the structure was partially closed for more than year.
Those same storms caused extensive damage in Aptos and Capitola, 70 miles south, where piers and waterfront infrastructure were swept away or damaged.
In 2024, a 150- to 180- foot section of the Santa Cruz wharf was ripped off by powerful waves.
At least 10 of the state’s dozens of coastal public piers were closed for part or all of 2024 due to structural damage sustained in winter storms since 2022. At least five others have longer-term upgrades planned to address structural issues.
“These things are costly to maintain,” said Zach Plopper, senior environmental director at Surfrider. “They are a part of our California coastal culture in many ways, but we’re going to need to reckon with, one, the state that they’re in, and two, the continuous and worsening threats they’re going to experience,”
He said most of the piers were constructed in the early 1900s, and they weren’t built to withstand decades of rough seas, storms and rising sea level.
“With this incoming El Niño, which is forecasted to be significant, and this marine heat wave we’re in the midst of, we’re kind of in uncharted waters as far as what this winter could bring in terms of storms and swells to the California coast, and we’re likely going to see a lot more damage,” he said. “Not just piers, but roads and other coastal infrastructure up and down the state.”
There was no storm in Pacifica earlier this week, so no single event could be blamed for the destruction.
However, a 2025 report from an outside engineering firm, GHD, found that several sections of the pier were in “poor” or “serious” condition, and they recommended closure before anticipated storms or events that could “subject the piles to high winds, swells and large waves.”
The firm found several areas of the pier where concrete was missing and rebar was exposed and corroding.
“The pier has continued to experience high winds and large waves in a harsh marine environment,” the engineers wrote in the report, noting that continuous exposure to seawater or marine spray was “detrimental” to the structure.
A 2023 city report estimated it would cost $19 million to repair.
That same year, a state law was enacted to require local governments along the California coast to plan for sea level rise in the coming decades.
Sea level has risen some 8 inches, on average, along the coast in the past 150 years, Plopper said, and researchers anticipate another foot in the next 25 years.
“We’re going to see profound shifts on our coastline, none that we have ever experienced before, and building static structures on the coast just doesn’t work all that well,” he said. “We’re going to have to make some really hard decisions.”
-

 Vermont2 minutes ago
Vermont2 minutes agoVermont Green FC plays Canada’s national soccer team in World Cup tuneup – VTDigger
-

 Virginia5 minutes ago
Virginia5 minutes agoNavy sailor sentenced to 44 years for killing fellow service member Angelina Resendiz in his Virginia barracks room
-

 Washington10 minutes ago
Washington10 minutes agoWhere to watch Washington Nationals vs San Francisco Giants: TV channel, start time, streaming for June 10
-

 Wisconsin17 minutes ago
Wisconsin17 minutes agoChris Borland heads back to Wisconsin as Hall of Fame inductee
-

 West Virginia20 minutes ago
West Virginia20 minutes agoWest Virginia Democrats re-elect Mike Pushkin, elect new leadership team – The Real WV
-

 Wyoming25 minutes ago
Wyoming25 minutes agoWyoming’s Most Treasured Views: Grand Teton National Park
-

 Crypto32 minutes ago
Crypto32 minutes ago‘De-Worsified, Not Diversified’: Robert Kiyosaki Warns Investors on a Hidden Risk
-

 Finance35 minutes ago
Finance35 minutes agoThe Future of Finance Jobs In The Age Of AI

