Science
Merck Sues Over Law Empowering Medicare to Negotiate With Drugmakers

The pharmaceutical company Merck on Tuesday sued the government over a federal law that empowers Medicare for the first time to negotiate prices directly with drugmakers.
Merck’s lawsuit, filed in federal court in Washington, is the drug industry’s most significant move so far to fight back against a substantial change to health policy, which will go into effect starting in 2026. Democrats pushed through the Medicare-negotiation program last summer as a provision of the Inflation Reduction Act, framing it as a way of lowering drug prices.
Only some drugs will be subject to negotiation with Medicare and only after they have been on the market without competition for years. But Merck, which generated $14.5 billion in profit last year, claimed in a statement on Tuesday that the law would stifle its ability and that of its peers to make risky investments in new cures.
Other drug companies have suggested that they will choose to cut certain drug development programs because of the projected dent to their revenue. Several have already said they were reassessing their research plans.
Merck said it was seeking a court order or another legal remedy that could exempt Merck from having to participate in the negotiation program.
In the complaint filed Tuesday, the company’s lawyers at the law firm Jones Day claim that the Medicare-negotiation program is unconstitutional. They claim that the program would coerce Merck to provide its products at government-set prices, violating a clause of the Fifth Amendment that prohibits the government from taking private property for public use without just compensation. They also claim that the program would violate Merck’s free-speech rights by coercing the company to sign an agreement it did not agree with upon the conclusion of the negotiation.
But several experts who study the industry said the constitutionality arguments were weak and would face an uphill battle in court. “What Merck argues is ‘coercion’ is actually the establishment of a freer, more rational marketplace” that will address a crucial root cause of high drug prices, said Dr. Ameet Sarpatwari, an expert in pharmaceutical policy at Harvard Medical School.
Experts noted that the negotiation process gives drug makers leeway to reject Medicare’s final offer and walk away without a deal if they are not happy, subject to a tax.
In September, the government plans to announce the first 10 drugs that will be subject to negotiation in 2026. A widely used Merck drug for diabetes known as Januvia is likely to be on that list.
The program could also affect Merck’s long-term plans for its golden goose, the blockbuster cancer drug Keytruda. It could be among the first products targeted when negotiations begin in 2028 on drugs administered in a health care setting.
The current version of Keytruda, administered as an infusion, will face its first competition that same year, so its sales are expected to erode regardless of whether it is targeted by the program. But Merck had been expecting to bring in significant revenue from a new formulation of Keytruda it is developing that can be more easily given under the skin. That could be subject to negotiation, too, under the government’s plans for the program.
The White House did not have any immediate comment on Merck’s lawsuit.
Sheryl Gay Stolberg contributed reporting.


Power is invisible, but its effects can be seen everywhere — especially in the health records of active duty military personnel.
By examining details of 1.5 million emergency room visits at U.S. military hospitals nationwide, researchers found that doctors invested significantly more resources in patients who outranked them than in patients of equal or lesser rank. The additional clinical effort devoted to powerful patients came at the expense of junior patients, who received worse care and were more likely to become seriously ill.
Military rank wasn’t the only form of power that translated into inequitable treatment. The researchers documented that patients fared better when they shared the same race or gender as their doctor, a pattern that tended to favor white men and caused Black patients in particular to be shortchanged by their physicians.
The results were published Thursday in the journal Science.
The findings have implications far beyond the realm of the military, said Manasvini Singh, a health and behavioral economist at Carnegie Mellon University who conducted the research with Stephen D. Schwab, an organizational health economist at the University of Texas at San Antonio.
For instance, they can help explain why Black students do better in school when they are taught by Black teachers, and why Black defendants get more even-handed treatment from Black judges.
“We think our results speak to many settings,” Singh said.
The disparities wrought by power imbalances are easy to spot but difficult to study in real-world scenarios.
“It’s just hard to measure power,” Singh said. “It’s abstract, it’s complicated.”
That’s where the military health records come in.
The Military Health System operates 51 hospitals across the country. The doctors who staff them are active-duty personnel, as are many of the patients they treat. Comparing their ranks gave Singh and Schwab a handy way to gauge the power differential between physicians and the people in their care.
The researchers restricted their analysis to patients who sought treatment in emergency departments, where patients are randomly assigned to doctors. That randomness made it easier to measure how power influenced the treatment patients received.
To further isolate the effects of power, the researchers made comparisons between patients of the same rank. If they happened to outrank their doctor, they were considered a “high-power” patient. If not, they were classified as a “low-power” patient.
The medical records showed that doctors put 3.6% more effort into treating high-power patients than low-power ones. They also utilized significantly more resources such as clinical tests, scans and procedures, according to the study.
Those extra resources translated into better care: High-power patients were 15% less likely to become sick enough to be admitted to the hospital over the next 30 days.
To see if they could replicate their results, Singh and Schwab narrowed their focus to doctors who treated patients within a one-year period before or after the patients were promoted to a higher rank. The researchers found that doctors devoted 1% more effort to patients post-promotion, as well as more medical resources. Those differences may have been small, but they were statistically significant, Schwab said.
Next, the pair considered what happened to low-power patients while high-power patients were getting extra attention. One hypothesis was that ordering additional tests for one patient might prompt doctors to order the same tests for everyone they treated that day. It was also possible that the decisions doctors made for their high-power patients had no bearing on their other patients.
Neither turned out to be the case. Instead, the added effort spent on high-power patients was siphoned away from low-power patients, who got 1.9% less effort from their doctors. On top of that, their risk of needing to return to the ER or be admitted to the hospital over the following 30 days increased by 3.4%, the researchers found.
“The powerful unwittingly ‘steal’ resources from less-powerful individuals,” Schwab and Singh wrote.
Outside the military, doctors and patients can’t use official rank to measure their power relative to each other, but they do contend with the effects of race and gender. That led the researchers to investigate whether the physicians in their study treated patients differently if they shared these attributes.
White doctors devoted more effort to white patients than to Black patients across the board, the researchers found. The gap was the same regardless of whether the doctor had a higher or lower rank than the patient.
However, white doctors increased their effort for high-power patients by the same amount regardless of race. As a result, white doctors treated high-power Black patients the same, on average, as low-power white patients.
The story was different for Black doctors. When they outranked their patients, they gave essentially the same amount of effort to everyone. But on the rare occasions when they encountered a higher-ranked Black patient, the amount by which they dialed up their efforts was more than 17 times greater than it was when they treated a higher-ranked white patient.
It’s not clear what accounted for this “off-the-charts effort,” the researchers wrote. They speculated that since Black service members were underrepresented among the pool of high-power patients, Black doctors were particularly attuned to their status.
The effects of gender were more difficult to ascertain, since biology dictates that men and women require different kinds of care.
Both male and female doctors invested the most effort in female patients who outranked them. But male doctors upgraded their care for high-power patients of both genders to a much greater extent than female doctors. And unlike female doctors, male doctors devoted more effort to female patients across the board.
Finally, the researchers wondered whether doctors gave preferential treatment to high-power patients because of their elevated status or because those patients had the authority to make trouble if they were unsatisfied with their care. To make inferences about this, they compared the treatment of retirees (who retained their status but had given up their authority) to the treatment of active-duty patients (who still had both).
Schwab and Singh found that high-power patients continued to elicit extra effort from doctors for up to five years after they retired, suggesting that status was an important factor.
“I think it’s really, really cool that even after retirement, you still have these effects,” said Joe C. Magee, a professor of management and organization at the NYU Stern School of Business who studies the role of hierarchy. He sees that as a strong sign that status was driving doctors’ decisions all along.
“What these folks are able to show is that it has real health consequences,” Magee said.
Eric Anicich, a professor of management and organization at the USC Marshall School of Business, called the study “impressive” and the findings “important.”
Although a 3.5% increase or a 1.9% decrease in physician effort may seem small, their cumulative impact is meaningful, especially when it comes to something as critically important as healthcare, he said.
The inequities documented in the study aren’t unique to doctors or to the armed forces, Schwab and Singh said. The mathematical model they developed to describe the behavior in military emergency rooms also helps explain why people in all kinds of situations give preferential treatment to people who look like them: It may help minimize the effects of societal disparities.
In a commentary that accompanies the study, Laura Nimmon of the University of British Columbia’s Centre for Health Education Scholarship wrote that “the ephemeral and unobservable nature of power has made it profoundly difficult to study.” But she said it’s worth the effort to make sure doctors wield their power more fairly.
The disparities reported by Schwab and Singh are “of serious concern to society at large,” she wrote.

As researchers increasingly rely on wastewater testing to monitor the spread of bird flu, some are questioning the reliability of the tests being used. Above, the Hyperion Water Reclamation Plant in Playa Del Rey.
(Jason Armond / Los Angeles Times)
As health officials turn increasingly toward wastewater testing as a means of tracking the spread of H5N1 bird flu among U.S. dairy herds, some researchers are raising questions about the effectiveness of the sewage assays.
Although the U.S. Centers for Disease Control and Prevention says current testing is standardized and will detect bird flu, some researchers voiced skepticism.
“Right now we are using these sort of broad tests” to test for influenza A viruses in wastewater, said epidemiologist Denis Nash, referring to a category of viruses that includes normal human flu and the bird flu that is circulating in dairy cattle, wild birds, and domestic poultry.
“It’s possible there are some locations around the country where the primers being used in these tests … might not work for H5N1,” said Nash, distinguished professor of epidemiology and executive director of City University of New York’s Institute for Implementation Science in Population Health.
The reason for this is that the tests most commonly used — polymerase chain reaction, or PCR, tests — are designed to detect genetic material from a specific organism, such as a flu virus.
But in order for them to identify the virus, they must be “primed” to know what they are looking for. Depending on what part of the virus researchers are looking for, they may not identify the bird flu subtype.
There are two common human influenza A viruses: H1N1 and H3N2. The “H” stands for hemagglutinin, which is an identifiable protein in the virus. The “N” stands for neuraminidase.
The bird flu, on the other hand, is also an influenza A virus. But it has the subtype H5N1.
That means that while the human and avian flu virus share the N1 signal, they don’t share an H.
If a test is designed to look for only the H1 and H3 as indicators of influenza A virus, they’re going to miss the bird flu.
Marc Johnson, a professor of molecular microbiology and immunology at the University of Missouri, said he doesn’t think that’s too likely. He said the generic panels that most labs use will capture H1, H3 and H5.
He said while his lab specifically looks for H1 and H3, “I think we may be the only ones doing that.”
It’s been just in the last few years that health officials have started using wastewater as a sentinel for community health.
Alexandria Boehm, professor of civil and environmental engineering at Stanford University and principal investigator and program director for WastewaterSCAN, said wastewater surveillance really got going during the pandemic. It’s become a routine way to look for hundreds if not thousands of viruses and other pathogens in municipal wastewater.
“Three years or four years ago, no one was doing it,” said Boehm, who collaborates with a network of researchers at labs at Stanford, Emory University and Alphabet Inc.’s life sciences research organization. “It sort of evolved in response to the pandemic and has continued to evolve.”
Since late March, when the bird flu was first reported in Texas dairy cattle, researchers and public health officials have been combing through wastewater samples. Most are using the influenza A tests they had already built into their systems — most of which were designed to detect human flu viruses, not bird flu.
On Tuesday, the CDC released its own dashboard showing wastewater sites where it has detected influenza A in the last two weeks.
Displaying a network of more than 650 sites across the nation, there were only three sites — in Florida, Illinois and Kansas — where levels of influenza A were considered high enough to warrant further agency investigation. There were more than 400 where data were insufficient to allow a determination.
Jonathan Yoder, deputy director of the CDC’s Division of Infectious Disease Readiness and Innovation, said those sites were deemed to have insufficient data because testing hasn’t been in place long enough, or there may not have been enough positive influenza A samples to include.
Asked if some of the tests being used could miss bird flu because of the way they were designed, he said: “We don’t have any evidence of that. It does seem like we’re at at a broad enough level that we don’t have any evidence that we would not pick up H5.”
He also said the tests were standardized across the network.
“I’m pretty sure that it’s the same assay being used at all the sites,” he said. “They’re all based on … what the CDC has published as a clinical assay for for influenza A, so it’s based on clinical tests.”
But there are discrepancies between the CDC’s findings and others’.
Earlier this week, a team of scientists from Baylor College of Medicine, the University of Texas Health Science Center at Houston, the Texas Epidemic Health Institute and the El Paso Water Utility, published a report showing high levels of bird flu from wastewater in nine Texas cities. Their data show that H5N1 is the dominant form of influenza A swirling in these Texas towns’ wastewater.
But unlike other research teams, including the CDC, they used an “agnostic” approach known as hybrid-capture sequencing.
“So it’s not just targeting one virus or one of several viruses,” as one does with PCR testing, said Eric Boerwinkle, dean of the UTHealth Houston School of Public Health and a member of the Texas team. “We’re actually in a very complex mixture, which is wastewater, pulling down viruses and sequencing them.”
“What’s critical here is it’s very specific to H5N1,” he said, noting they’d been doing this kind of testing for approximately two years, and hadn’t ever seen H5N1 before the middle of March.
Blake Hanson, an assistant professor at the University of Texas Health Science Center at Houston School of Public Health and a member of the Texas wastewater team, agreed, saying that PCR-based methods are “exquisite” and “highly accurate.”
“But we have the ability to look at the representation of the entire genome, not just a marker component of it. And so that has allowed us to look at H5N1, differentiate it from some of our seasonal fluids like H1N1 and H3N2,” he said. “It’s what gave us high confidence that it is entirely H5N1, whereas the other papers are using a part of the H5 gene as a marker for H5.”
Boerwinkle and Hanson underscored that while they could identify H5N1 in the wastewater, they cannot tell where it came from.
“Texas is really a confluence of a couple of different flyways for migratory birds, and Texas is also an agricultural state, despite having quite large cities,” Boerwinkle said. “It’s probably correct that if you had to put your dime and gamble what was happening, it’s probably coming from not just one source but from multiple sources. We have no reason to think that one source is more likely any one of those things.”
But they are pretty confident it’s not coming from people.
“Because we are looking at the entirety of the genome, when we look at the single human H5N1 case, the genomic sequence … has a hallmark amino acid change … compared to all of the cattle from that same time point,” Hanson said. “We do not see that hallmark amino acid present in any of our sequencing data. And we’ve looked very carefully for that, which gives us some confidence that we’re not seeing human-human transmission.”
The Texas’ team approach was really exciting, said Devabhaktuni Srikrishna, the CEO and founder of PatientKnowHow.com, noting it exhibited “proof of principle” for employing this kind of metagenomic testing protocol for wastewater and air.
He said government agencies, private companies and academics have been searching for a reliable way to test for thousands of microscopic organisms — such as pathogens — quickly, reliably and at low cost.
“They showed it can be done,” he said.

Deaths from drug overdoses fell last year in the United States as fewer people lost their lives to fentanyl and other opioids, marking the first time the death toll had dropped in five years, according to newly released estimates from the Centers for Disease Control and Prevention.
Federal officials said the numbers show a 3% decline in the estimated overdose fatalities between 2022 and 2023. That downturn equates to nearly 3,500 fewer deaths across the U.S. than the year before.
The new figures are tentative and could still be updated. Even a slight decline could be a balm for a country where drug overdoses have taken a devastating toll: In one survey, more than 40% of adults said they knew someone who lost their life to a drug overdose, according to a Rand study published this year.
“I’m thrilled that there wasn’t an increase, but we’re still talking about 107,000 people dying, which is completely unacceptable,” said Beau Kilmer, co-director of the Rand Drug Policy Research Center. Kilmer said better data on drug use are needed to untangle exactly what is driving the changes.
Community groups and health officials grappling with the devastating toll of fentanyl have pushed to equip more people with naloxone, a medicine that can stop opioid overdoses and is commonly sold as a nasal spray under the brand name Narcan. Los Angeles County officials, for instance, credited an effort to hand out Narcan on the streets when they announced last week that overdose deaths had stopped surging among homeless people. To try to reduce the deadly risks, people who use drugs have also turned to test strips to detect fentanyl and avoided using drugs by themselves, among other strategies.
Health researchers have also noted that broader changes in the population could be affecting the numbers: Many heroin users who switched to fentanyl have died, and if fewer people are newly turning to fentanyl use, that could mean fewer people are now at risk, said Dr. Daniel Ciccarone, a UCSF addiction medicine professor.
“Based on utterly anecdotal, street-level observations, I’ll say there aren’t a lot of newbies,” Ciccarone said. “We’re looking for them, but we don’t see them. We don’t see the 22-year-old who says, ‘Hey, I want to use fentanyl.’ This is an aging cohort.”
Even as U.S. deaths linked to fentanyl and other opioids dropped between 2022 and 2023, the country saw an uptick in deaths tied to stimulants such as methamphetamine and cocaine, according to the new estimates. Drug researchers said that in recent years, many deaths involving meth have also involved opioids.
And not all parts of the country saw an overall drop in fatal overdoses. “In the East Coast and in the Midwest, we are seeing declines, but on the West Coast — particularly in the upper Northwest — we’re still seeing increases,” said Farida Ahmad, a health scientist at the National Center for Health Statistics.
The federal figures show that in California, the estimated number of overdose deaths continued to rise in 2023 compared with 2022, increasing by 4.1%. In Oregon and Washington, increases were significantly steeper — roughly 30% and 27% respectively.
Drug use can differ from region to region, shaping ensuing overdoses and deaths: Fentanyl hit the eastern U.S. before spreading west, and methamphetamine use generally has been more common on the West Coast.
Ciccarone lamented that the West Coast should have been better prepared for fentanyl after seeing it hit other parts of the country years earlier, calling it a “failure of public policy.”
“We saw this coming. So why didn’t we prepare for it better?”
Ciccarone credited states in the Midwest and East Coast that had seen notable decreases in overdose deaths, saying that although the exact reasons are unclear, there has been a panoply of efforts that could play a role, including ramping up naloxone distribution and easing access to buprenorphine to treat opioid addiction.
“These are places that were hard hit by fentanyl,” Ciccarone said. “So they’re doing something right.”
The federal estimates released Wednesday do not detail how many deaths linked to methamphetamine also involved other drugs, a phenomenon that has gained growing attention as American mix drugs both knowingly and unknowingly.
Researchers drawing on both federal and local data have found substantial overlap in methamphetamine and opioid use: In L.A. County, for instance, a recent report indicated that in 2022, nearly half of overdose deaths among homeless people involved both methamphetamine and fentanyl.
People who use fentanyl may turn to stimulants for energy to get themselves through daily activities, said Chelsea Shover, an assistant professor at UCLA’s David Geffen School of Medicine. For those facing the dangers of living outside, “you know what helps you stay up at night and stay vigilant? Meth.”
Shover said in recent years, national data have consistently shown the majority of methamphetamine deaths also involve opioids. Those findings were echoed in local research by Shover and other researchers, which found that between 2012 and mid-2021, the bulk of meth-related deaths in L.A. County also involved other drugs or medical conditions, rather than being driven solely by the stimulant.
To help prevent such deaths, “we need to keep doing what we’re doing for opioid-related deaths — because a lot of meth-involved deaths are also opioid-involved,” Shover said.
Scholars have also urged more attention to methamphetamine itself: As it stands, there are no medications approved by the Food and Drug Administration to treat addiction to meth, although some existing medicines have shown promising results, as has offering incentives such as gift cards for people to stay off stimulants.
“The massive investment in reducing overdose deaths has been almost exclusively targeted to opioids,” said Steven Shoptaw, director of the UCLA Center for Behavioral and Addiction Medicine. “There’s been no systematic investment to reduce methamphetamine deaths” — a lapse that Shoptaw said had hindered effective interventions from being widely adopted.
Americans have been eager for any signs of hope amid the overdose crisis, but experts have cautioned against declaring victory too soon in reaction to year-to-year changes in overdose deaths.
For instance, University of Pittsburgh researchers found that the last time fatal overdoses dropped nationally in 2018, the downturn coincided with stricter regulations in China on carfentanil, a highly potent synthetic opioid. The following year, deaths from drug overdoses rose again.
Dr. Donald Burke said that the estimated number of overdose deaths in 2023 was still above the level that researchers had forecast, based on the historic trajectory of such fatalities. The death numbers had jumped higher than expected during the COVID-19 pandemic, Burke said — and may just be returning to the same levels that would have happened in its absence.
“You can make a case that it’s come down, but it’s come down because the COVID impact is less now,” said Burke, dean emeritus of the University of Pittsburgh School of Public Health.
“Without knowing what are the drivers, it’s really hard to tell whether a reduction is a return to the expected trajectory or some other change,” said Dr. Hawre Jalal, an associate professor at the University of Ottawa who has partnered with Burke on such research.
Ciccarone was reluctant to even characterize the newly released estimates as a decrease in overdose deaths, instead referring to “a flattening of the curve.”
“Can we sing hosannas over that? No,” Ciccarone said. “We’re still fighting. We still have a lot of work to do to bend this overdose curve down.”

Ignite Nebraska tackling metro talent shortage with new program

Trip Report: 11,161' Mt. Scowden's “Dog Leg Chute” | Sierra Nevada Mountains, CA – SnowBrains

4-year-old child bitten by rabid fox in Hollis, NH; animal euthanized – Boston News, Weather, Sports | WHDH 7News

Gold bars in baggies and cash crammed in boots: Prosecutors detail Menendez's hoarded riches • New Jersey Monitor

KCBD Investigates: FBI report details new information in New Mexico murder, kidnapping case

See it: Tesla crashes into Columbus convention center at 70 mph

Colorado Rockies game no. 116 thread: Zac Gallen vs José Ureña

Fox News Politics: Georgia the whole day through

Death of missing Oregon girl found in stream ruled homicide

At least 2 dead as tornadoes hit Alabama, damage homes across Southeast

Read the Texas Governor’s Pardon

Alaska lawmakers end their session with late bills passing on energy, education

Taiwan grapples with divisive history as new president prepares for power
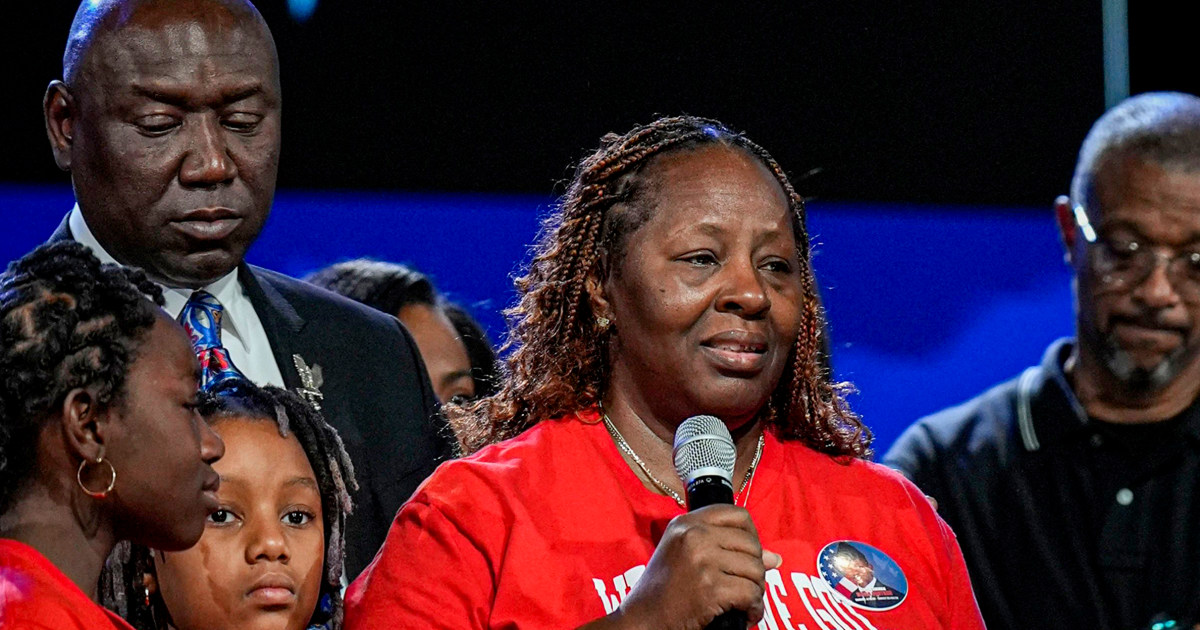
Lawyer for family of slain airman says Florida deputy call shows he went to wrong apartment

Illegal immigrants from foreign adversary hit new high amid national security fears: 'Extremely alarming'
-
 Politics1 week ago
Politics1 week agoBiden takes role as bystander on border and campus protests, surrenders the bully pulpit
-
 Politics1 week ago
Politics1 week ago'You need to stop': Gov. Noem lashes out during heated interview over book anecdote about killing dog
-
 Politics1 week ago
Politics1 week agoRFK Jr said a worm ate part of his brain and died in his head
-
 News1 week ago
News1 week agoMan, 75, confesses to killing wife in hospital because he couldn’t afford her care, court documents say
-
 World1 week ago
World1 week agoPentagon chief confirms US pause on weapons shipment to Israel
-
 Politics1 week ago
Politics1 week agoHere's what GOP rebels want from Johnson amid threats to oust him from speakership
-
 World1 week ago
World1 week agoPro-Palestine protests: How some universities reached deals with students
-
 World1 week ago
World1 week agoConvicted MEP's expense claims must be published: EU court