Science
Tooth decay still plagues California kids nearly a decade after Medi-Cal promised change

Eight years after an independent state watchdog agency harshly criticized the state for failing to provide dental care to low-income children, California has failed to remedy the problem or fully implement the commission’s recommendations, according to a follow-up review published last week.
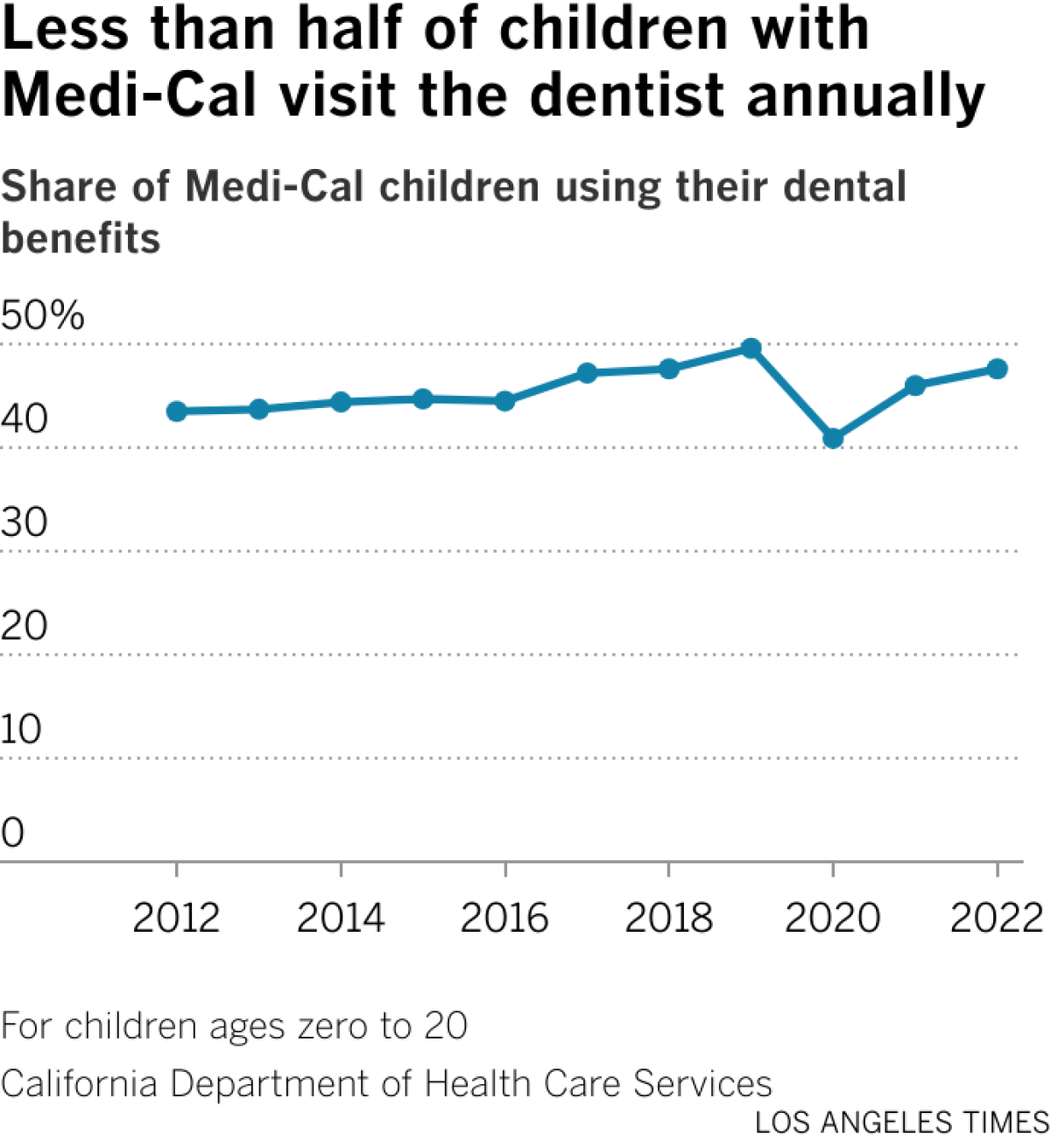
The Little Hoover Commission found that less than half of the children in Medi-Cal received an annual dental visit in 2022 — 3% higher than when the initial report was released in 2016, which implored the state to do more to ensure that children have access to needed care.
“California is still doing a miserable job,” said Pedro Nava, chair of the commission and a former member of the state Assembly. “We have failed generations of children. We and they deserve better.”
The 2016 report was one of the most scathing reports that the commission had generated in years, Nava said. It found that only 44.5% of children in the Medi-Cal program had a visit with a dentist in 2016, a key indicator of whether children are receiving the care they need to prevent painful dental decay, and recommended that the state increase the rate to 66%. Lawmakers responded with a law requiring the health department to set a target of at least 60% of children.
Last fall, after the publication of an L.A. Times story on high rates of dental disease among California children, the commission initiated a follow-up review of the state’s progress.
It found that the state had fallen far short of the goal; in 2022, the most recent data provided in the report, 47.6% of children with Medi-Cal visited a dentist, a 3-percentage-point increase from 2016.
“If you were an investor in a private company, and that was the best they could do, you’d sell your stock and invest it somewhere else,” Nava said. “It is a disappointment that low-income families with children have to shoulder the burden of this every day.”
Engage with our community-funded journalism as we delve into child care, transitional kindergarten, health and other issues affecting children from birth through age 5.
California has made some improvements since 2016, the report said, fully implementing one recommendation and partially implementing seven of the commission’s eight others.
The state health department, however, disputes those findings and said they have fully implemented all of the recommendations from the 2016 report. The percentage of kids going to the dentist had been increasing significantly, they said — up to 49.6% in 2019 — but the pandemic interrupted that growth.
“California, along with every other state in the nation, was profoundly impacted by the effects of the COVID-19 pandemic. Virtually every state within the U.S. decreased and had a recovery period that lasted at least two years to return to pre-COVID figures,” the Department of Health Care Services wrote in a statement provided to The Times.
Since 2016, the department has made a number of important changes, the department wrote, including expanding the use of tele-dentistry to reach members across the state, increasing provider networks and creating a public education and outreach media campaign for Medi-Cal patients and providers.
In 2023 the percentage of children who visited the dentist “recovered to 2019 levels. Even higher utilization is projected in 2024,” the health department said, although data have not been been released on this upward trend.
“I don’t think this response really questions the fact that they have not come close to reaching the recommendation set by the Legislature of 60% of kids getting in to see the dentist, let alone our rate of 66%,” said Ethan Rarick, executive director of the Little Hoover Commission. “Kids’ dental health is among the worst in the country, and much more needs to be done.”
California children have among the worst rates of dental disease in the nation. A national survey from 2020 to 2021 found that 14.8% of the state’s children ages 1 to 17 had decayed teeth or cavities in the last 12 months studied — ranking 47th out of 51 among all the states and the District of Columbia, with only Louisiana and Wyoming faring worse. “I don’t understand,” Nava said. “If you’re the fifth-largest economy in the world, you ought to be a leader in children’s health.”
Nationwide, more than half of children develop cavities by the age of 8, usually because of poor nutrition, bad hygiene habits or a lack of dental care.
The reality of dental disease can be devastating to children, causing pain and difficulty eating, sleeping and focusing in school, and low-income children of color are at greatest risk. L.A. County’s Smile Survey, which was conducted by the public health department, found that on any given day, more than 4,500 Los Angeles County kindergarten and third-grade children need urgent dental care, which means they may be experiencing mouth pain or a serious infection.
The state increased the payment rate for evaluating a child’s teeth, for example, from $15 to $45, and up to $100 if a dentist sees the same child two years in a row, according to the California Dental Assn. The reimbursement for a filling increased from $48 to $67.20. These rate increases were funded by Proposition 56, a 2016 tobacco tax that raised money for Medi-Cal payments, and by CalAIM, a state initiative to transform Medi-Cal. The Proposition 56 money was also used to fund county oral health plans and repay student loans for new dentists.
The state has made it easier for dentists to enroll as Medi-Cal providers by simplifying the enrollment forms and putting them online, the report said. It also began a pilot program for telehealth to help bring care to healthcare deserts through the Dental Transformation Initiative.
Between the Medi-Cal payment rate and fewer administrative burdens, dentists appear to have taken note: 40% of all California dentists in the state now take Medi-Cal, a 34% increase since 2017, according to the dental association.
“The program had such a huge hole to dig out of, and COVID really derailed everything,” said Brianna Pittman-Spencer, senior director of government affairs at the California Dental Assn. “There have been improvements but obviously still a long way to go for the impact we want.”
Eileen Espejo, who leads the oral health project at Children Now, said she was pleased to see that the state had at least started to implement most of the recommendations, but that the numbers suggest the approach may not be working. “If we’re going to do better, it doesn’t seem like we should do more than the same,” she said.
In particular, she worries about children in far northern counties and those bordering Nevada, where dentists are hard to find. Twenty-one counties have five or fewer dental providers that take Medi-Cal, the report found. “How are we going to get providers to live in parts of the state where they aren’t yet?” she asked, adding that using more telehealth dentistry and allowing dental hygienists to provide more care could be part of the solution.
“Hopefully this report will light a fire and get more people engaged,” Espejo said. “I certainly think it opens the pathway for advocates to ask for more resources to help improve the program.”
This article is part of The Times’ early childhood education initiative, focusing on the learning and development of California children from birth to age 5. For more information about the initiative and its philanthropic funders, go to latimes.com/earlyed.







Science
Commentary: My toothache led to a painful discovery: The dental care system is full of cavities as you age

I had a nagging toothache recently, and it led to an even more painful revelation.
If you X-rayed the state of oral health care in the United States, particularly for people 65 and older, the picture would be full of cavities.
“It’s probably worse than you can even imagine,” said Elizabeth Mertz, a UC San Francisco professor and Healthforce Center researcher who studies barriers to dental care for seniors.
Mertz once referred to the snaggletoothed, gap-filled oral health care system — which isn’t really a system at all — as “a mess.”
But let me get back to my toothache, while I reach for some painkiller. It had been bothering me for a couple of weeks, so I went to see my dentist, hoping for the best and preparing for the worst, having had two extractions in less than two years.
Let’s make it a trifecta.
My dentist said a molar needed to be yanked because of a cellular breakdown called resorption, and a periodontist in his office recommended a bone graft and probably an implant. The whole process would take several months and cost roughly the price of a swell vacation.
I’m lucky to have a great dentist and dental coverage through my employer, but as anyone with a private plan knows, dental insurance can barely be called insurance. It’s fine for cleanings and basic preventive routines. But for more complicated and expensive procedures — which multiply as you age — you can be on the hook for half the cost, if you’re covered at all, with annual payout caps in the $1,500 range.
“The No. 1 reason for delayed dental care,” said Mertz, “is out-of-pocket costs.”
So I wondered if cost-wise, it would be better to dump my medical and dental coverage and switch to a Medicare plan that costs extra — Medicare Advantage — but includes dental care options. Almost in unison, my two dentists advised against that because Medicare supplemental plans can be so limited.
Sorting it all out can be confusing and time-consuming, and nobody warns you in advance that aging itself is a job, the benefits are lousy, and the specialty care you’ll need most — dental, vision, hearing and long-term care — are not covered in the basic package. It’s as if Medicare was designed by pranksters, and we’re paying the price now as the percentage of the 65-and-up population explodes.
So what are people supposed to do as they get older and their teeth get looser?
A retired friend told me that she and her husband don’t have dental insurance because it costs too much and covers too little, and it turns out they’re not alone. By some estimates, half of U.S. residents 65 and older have no dental insurance.
That’s actually not a bad option, said Mertz, given the cost of insurance premiums and co-pays, along with the caps. And even if you’ve got insurance, a lot of dentists don’t accept it because the reimbursements have stagnated as their costs have spiked.
But without insurance, a lot of people simply don’t go to the dentist until they have to, and that can be dangerous.
“Dental problems are very clearly associated with diabetes,” as well as heart problems and other health issues, said Paul Glassman, associate dean of the California Northstate University dentistry school.
There is one other option, and Mertz referred to it as dental tourism, saying that Mexico and Costa Rica are popular destinations for U.S. residents.
“You can get a week’s vacation and dental work and still come out ahead of what you’d be paying in the U.S.,” she said.
Tijuana dentist Dr. Oscar Ceballos told me that roughly 80% of his patients are from north of the border, and come from as far away as Florida, Wisconsin and Alaska. He has patients in their 80s and 90s who have been returning for years because in the U.S. their insurance was expensive, the coverage was limited and out-of-pocket expenses were unaffordable.
“For example, a dental implant in California is around $3,000-$5,000,” Ceballos said. At his office, depending on the specifics, the same service “is like $1,500 to $2,500.” The cost is lower because personnel, office rent and other overhead costs are cheaper than in the U.S., Ceballos said.
As we spoke by phone, Ceballos peeked into his waiting room and said three patients were from the U.S. He handed his cellphone to one of them, San Diegan John Lane, who said he’s been going south of the border for nine years.
“The primary reason is the quality of the care,” said Lane, who told me he refers to himself as 39, “with almost 40 years of additional” time on the clock.
Ceballos is “conscientious and he has facilities that are as clean and sterile and as medically up to date as anything you’d find in the U.S.,” said Lane, who had driven his wife down from San Diego for a new crown.
“The cost is 50% less than what it would be in the U.S.,” said Lane, and sometimes the savings is even greater than that.
Come this summer, Lane may be seeing even more Californians in Ceballos’ waiting room.
“Proposed funding cuts to the Medi-Cal Dental program would have devastating impacts on our state’s most vulnerable residents,” said dentist Robert Hanlon, president of the California Dental Assn.
Dental student Somkene Okwuego smiles after completing her work on patient Jimmy Stewart, 83, who receives affordable dental work at the Ostrow School of Dentistry of USC on the USC campus in Los Angeles on February 26, 2026.
(Genaro Molina / Los Angeles Times)
Under Proposition 56’s tobacco tax in 2016, supplemental reimbursements to dentists have been in place, but those increases could be wiped out under a budget-cutting proposal. Only about 40% of the state’s dentists accept Medi-Cal payments as it is, and Hanlon told me a CDA survey indicates that half would stop accepting Medi-Cal patients and many others will accept fewer patients.
“It’s appalling that when the cost of providing healthcare is at an all-time high, the state is considering cutting program funding back to 1990s levels,” Hanlon said. “These cuts … will force patients to forgo or delay basic dental care, driving completely preventable emergencies into already overcrowded emergency departments.”
Somkene Okwuego, who as a child in South L.A. was occasionally a patient at USC’s Herman Ostrow School of Dentistry clinic, will graduate from the school in just a few months.
I first wrote about Okwuego three years ago, after she got an undergrad degree in gerontology, and she told me a few days ago that many of her dental patients are elderly and have Medi-Cal or no insurance at all. She has also worked at a Skid Row dental clinic, and plans after graduation to work at a clinic where dental care is free or discounted.
Okwuego said “fixing the smiles” of her patients is a privilege and boosts their self-image, which can help “when they’re trying to get jobs.” When I dropped by to see her Thursday, she was with 83-year-old patient Jimmy Stewart.
Stewart, an Army veteran, told me he had trouble getting dental care at the VA and had gone years without seeing a dentist before a friend recommended the Ostrow clinic. He said he’s had extractions and top-quality restorative care at USC, with the work covered by his Medi-Cal insurance.
I told Stewart there could be some Medi-Cal cuts in the works this summer.
“I’d be screwed,” he said.
Him and a lot of other people.
steve.lopez@latimes.com

Central Coast Water authorities approved waste discharge permits for Diablo Canyon nuclear plant Thursday, making it nearly certain it will remain running through 2030, and potentially through 2045.
The Pacific Gas & Electric-owned plant was originally supposed to shut down in 2025, but lawmakers extended that deadline by five years in 2022, fearing power shortages if a plant that provides about 9 percent the state’s electricity were to shut off.
In December, Diablo Canyon received a key permit from the California Coastal Commission through an agreement that involved PG&E giving up about 12,000 acres of nearby land for conservation in exchange for the loss of marine life caused by the plant’s operations.
Today’s 6-0 vote by the Central Coast Regional Water Board approved PG&E’s plans to limit discharges of pollutants into the water and continue to run its “once-through cooling system.” The cooling technology flushes ocean water through the plant to absorb heat and discharges it, killing what the Coastal Commission estimated to be two billion fish each year.
The board also granted the plant a certification under the Clean Water Act, the last state regulatory hurdle the facility needed to clear before the federal Nuclear Regulatory Commission (NRC) is allowed to renew its permit through 2045.
The new regional water board permit made several changes since the last one was issued in 1990. One was a first-time limit on the chemical tributyltin-10, a toxic, internationally-banned compound added to paint to prevent organisms from growing on ship hulls.
Additional changes stemmed from a 2025 Supreme Court ruling that said if pollutant permits like this one impose specific water quality requirements, they must also specify how to meet them.
The plant’s biggest water quality impact is the heated water it discharges into the ocean, and that part of the permit remains unchanged. Radioactive waste from the plant is regulated not by the state but by the NRC.
California state law only allows the plant to remain open to 2030, but some lawmakers and regulators have already expressed interest in another extension given growing electricity demand and the plant’s role in providing carbon-free power to the grid.
Some board members raised concerns about granting a certification that would allow the NRC to reauthorize the plant’s permits through 2045.
“There’s every reason to think the California entities responsible for making the decision about continuing operation, namely the California [Independent System Operator] and the Energy Commission, all of them are sort of leaning toward continuing to operate this facility,” said boardmember Dominic Roques. “I’d like us to be consistent with state law at least, and imply that we are consistent with ending operation at five years.”
Other board members noted that regulators could revisit the permits in five years or sooner if state and federal laws changes, and the board ultimately approved the permit.

The H5N1 bird flu virus that devastated South American elephant seal populations has been confirmed in seals at California’s Año Nuevo State Park, researchers from UC Davis and UC Santa Cruz announced Wednesday.
The virus has ravaged wild, commercial and domestic animals across the globe and was found last week in seven weaned pups. The confirmation came from the U.S. Department of Agriculture’s National Veterinary Services Laboratory in Ames, Iowa.
“This is exceptionally rapid detection of an outbreak in free-ranging marine mammals,” said Professor Christine Johnson, director of the Institute for Pandemic Insights at UC Davis’ Weill School of Veterinary Medicine. “We have most likely identified the very first cases here because of coordinated teams that have been on high alert with active surveillance for this disease for some time.”
Since last week, when researchers began noticing neurological and respoiratory signs of the disease in some animals, 30 seals have died, said Roxanne Beltran, a professor of ecology and evolutionary biology at UC Santa Cruz. Twenty-nine were weaned pups and the other was an adult male. The team has so far confirmed the virus in only seven of the dead pups.
Infected animals often have tremors convulsions, seizures and muscle weakness, Johnson said.
Beltran said teams from UC Santa Cruz, UC Davis and California State Parks monitor the animals 260 days of the year, “including every day from December 15 to March 1” when the animals typically come ashore to breed, give birth and nurse.
The concerning behavior and deaths were first noticed Feb. 19.
“This is one of the most well-studied elephant seal colonies on the planet,” she said. “We know the seals so well that it’s very obvious to us when something is abnormal. And so my team was out that morning and we observed abnormal behaviors in seals and increased mortality that we had not seen the day before in those exact same locations. So we were very confident that we caught the beginning of this outbreak.”
In late 2022, the virus decimated southern elephant seal populations in South America and several sub-Antarctic Islands. At some colonies in Argentina, 97% of pups died, while on South Georgia Island, researchers reported a 47% decline in breeding females between 2022 and 2024. Researchers believe tens of thousands of animals died.
More than 30,000 sea lions in Peru and Chile died between 2022 and 2024. In Argentina, roughly 1,300 sea lions and fur seals perished.
At the time, researchers were not sure why northern Pacific populations were not infected, but suspected previous or milder strains of the virus conferred some immunity.
The virus is better known in the U.S. for sweeping through the nation’s dairy herds, where it infected dozens of dairy workers, millions of cows and thousands of wild, feral and domestic mammals. It’s also been found in wild birds and killed millions of commercial chickens, geese and ducks.
Two Americans have died from the virus since 2024, and 71 have been infected. The vast majority were dairy or commercial poultry workers. One death was that of a Louisiana man who had underlying conditions and was believed to have been exposed via backyard poultry or wild birds.
Scientists at UC Santa Cruz and UC Davis increased their surveillance of the elephant seals in Año Nuevo in recent years. The catastrophic effect of the disease prompted worry that it would spread to California elephant seals, said Beltran, whose lab leads UC Santa Cruz’s northern elephant seal research program at Año Nuevo.
Johnson, the UC Davis researcher, said the team has been working with stranding networks across the Pacific region for several years — sampling the tissue of birds, elephant seals and other marine mammals. They have not seen the virus in other California marine mammals. Two previous outbreaks of bird flu in U.S. marine mammals occurred in Maine in 2022 and Washington in 2023, affecting gray and harbor seals.
The virus in the animals has not yet been fully sequenced, so it’s unclear how the animals were exposed.
“We think the transmission is actually from dead and dying sea birds” living among the sea lions, Johnson said. “But we’ll certainly be investigating if there’s any mammal-to-mammal transmission.”
Genetic sequencing from southern elephant seal populations in Argentina suggested that version of the virus had acquired mutations that allowed it to pass between mammals.
The H5N1 virus was first detected in geese in China in 1996. Since then it has spread across the globe, reaching North America in 2021. The only continent where it has not been detected is Oceania.
Año Nuevo State Park, just north of Santa Cruz, is home to a colony of some 5,000 elephant seals during the winter breeding season. About 1,350 seals were on the beach when the outbreak began. Other large California colonies are located at Piedras Blancas and Point Reyes National Sea Shore. Most of those animals — roughly 900 — are weaned pups.
It’s “important to keep this in context. So far, avian influenza has affected only a small proportion of the weaned at this time, and there are still thousands of apparently healthy animals in the population,” Beltran said in a press conference.
Public access to the park has been closed and guided elephant seal tours canceled.
Health and wildlife officials urge beachgoers to keep a safe distance from wildlife and keep dogs leashed because the virus is contagious.

Meyer’s Late Score Lifts Wyoming past Air Force – SweetwaterNOW

Crypto Sector Suffers Exodus of Reliable Retail Investors | PYMNTS.com

Canton High School students find success in personal finance

The Workout Habit That Can Become Harm

Film reviews: ‘How to Make a Killing,’ ‘Pillion,’ and ‘Midwinter Break’

Florida High School Football Rankings: Top 25 teams – Oct. 21

Cleary's 21 help Le Moyne down Central Connecticut State 69-64 in OT

How old is Bo Nix? What to know about Oregon quarterback ahead of 2024 NFL Draft

99th annual Pony Swim held in Virginia

Indiana Members Credit Union announced as new anchor tenant at Bottleworks District

House Republicans push Johnson to go to war with Senate over SAVE Act

Israel FM says Europe too divided, slams Spanish PM

Satellite images provide view inside Iran at war

Video: What the Texas Primary Battle Means for the Midterms

Dems’ potential 2028 hopefuls come out against US strikes on Iran
-

 World4 days ago
World4 days agoExclusive: DeepSeek withholds latest AI model from US chipmakers including Nvidia, sources say
-

 Massachusetts4 days ago
Massachusetts4 days agoMother and daughter injured in Taunton house explosion
-

 Montana1 week ago
Montana1 week ago2026 MHSA Montana Wrestling State Championship Brackets And Results – FloWrestling
-

 Denver, CO4 days ago
Denver, CO4 days ago10 acres charred, 5 injured in Thornton grass fire, evacuation orders lifted
-

 Louisiana7 days ago
Louisiana7 days agoWildfire near Gum Swamp Road in Livingston Parish now under control; more than 200 acres burned
-

 Technology1 week ago
Technology1 week agoYouTube TV billing scam emails are hitting inboxes
-

 Politics1 week ago
Politics1 week agoOpenAI didn’t contact police despite employees flagging mass shooter’s concerning chatbot interactions: REPORT
-

 Technology1 week ago
Technology1 week agoStellantis is in a crisis of its own making