Science
'I don't want him to go': An autistic teen and his family face stark choices

Christine LyBurtus was aching and fearful of what might happen when her 13-year-old son returned home.
Noah had been sent to Children’s Hospital of Orange County for a psychiatric hold lasting up to 72 hours after he punched at walls, flipped over a table, ripped out a chunk of his mother’s hair and tried to break a car window.
“There’s nothing else to call it except a psychotic episode,” LyBurtus said.
The clock was ticking on that August day in 2022. The single mother wanted help to prevent such an episode from happening again, maybe with a different medication. Hospital staff were waiting for a psychiatric bed, possibly at another hospital with a dedicated unit for patients with autism or other developmental disabilities.
But as the hours ran out on the hold, it became clear that wasn’t happening. LyBurtus brought Noah home to their Fullerton apartment.
“When he came back home, it kind of broke my heart,” said his sister, Karissa, who is two years older. “He looked like, ‘What the heck did you guys put me into?’”
Christine LyBurtus makes a snack for Noah.
(Allen J. Schaben / Los Angeles Times)
The next night, Noah was back in the ER after smashing a television and attacking his mother. This time, he was transferred to a different hospital for three weeks, prescribed medications for psychosis, and then sent to a residential facility in Garden Grove.
LyBurtus said she was told it would be a stopgap measure — just for three weeks — until she could line up more help at home. But when she phoned to ask about visiting her son, LyBurtus said she was told she couldn’t see him for a month.
“He lives here now,” someone told her, she said, and the staff needed time to “break him in.”
LyBurtus felt like she was being pushed to give up her son, instead of getting the help her family needed. She insisted on bringing him home.
::
Autism is a developmental condition that can shape how people think, communicate, move and process sensory information. When Noah was 3, a doctor noted he was a “very cute little boy” who played alone, rocked back and forth, and sometimes bit himself. Noah’s eye contact was “fleeting.” He could speak about 20 words, but often cried or pulled his mother’s hand to communicate.
The physician summed up his behavior as “characteristic of a DSM-IV diagnosis of autistic disorder.”
When he was in elementary school, LyBurtus stopped working full time outside the home and enrolled in a state program that paid her as his caregiver. She relies on Medi-Cal for his medical care, and much of his schooling has been in Orange County-run programs for children with moderate to severe disabilities.
Noah does not speak but sometimes uses pictures, an app on a tablet, or some sign language to communicate. When a reporter visited their home last year, Noah bobbed his head and shoulders as he listened to music on his iPad. He flapped his hands as LyBurtus made him a peanut-butter-and-banana smoothie, and then dutifully followed her instructions to chuck the peel and put the almond milk away. It was a good day, LyBurtus said with relief.
But on other days, LyBurtus said her son could be rigid; his demands, unpredictable. “Some days he’s fixated on having three pairs of pants on … Some days he wants to take seven showers. The next day, I can’t get him to take showers.”

Christine LyBurtus greets Noah as he arrives home from school.
(Allen J. Schaben / Los Angeles Times)
When frustrated, Noah might erupt, banging his head against walls and trying to jump out the windows of their apartment. He had kicked and bitten his mother when she tried to redirect him. In the worst instances, LyBurtus had resorted to hiding in the bathroom — her “safe room” — and urged Karissa to lock herself in the bedroom.
As Noah grew taller and stronger, LyBurtus stripped bare the walls of her apartment to try to make it safe, installed shatterproof windows and removed a knob from a closet door to prevent Noah from using it as a foothold to scale over the top of the closet door. She made sure to flag her address for the Fullerton Police Department so it knew her son was developmentally disabled.
“I’m just so grateful that my son never got shot,” LyBurtus said.
Each of the 911 calls was the start of a Sisyphean routine. Noah “has been challenging to place in [a] mental health facility due to behavioral care needs with severe autism,” a doctor wrote when he was back at Children’s Hospital of Orange County yet again.

Noah leaps into the air inside his Fullerton home. At left is Terrence Morris, one of Noah’s caregivers.
(Mel Melcon / Los Angeles Times)
As the family tried to get through each crisis, LyBurtus was also facing a common struggle among parents of California children with disabilities: not getting the help they were supposed to receive from the state.
LyBurtus was getting assistance through a local regional center, one of the nonprofit agencies contracted by the California Department of Developmental Services. She said she’d been authorized to receive 40 hours weekly of respite care — meant to relieve families of children with disabilities for short periods — but was sometimes receiving only 12 to 16 hours.
She was also supposed to have two workers at a time, LyBurtus said, but caregivers were so scarce that she was scheduling one at a time in order to cover as many hours as she could.
In the meantime, Noah wasn’t sleeping and she was going through so much laundry detergent and quarters that her grocery budget was drained. At one point, she wanted to go to a food bank, but there would be no one to watch him.
“I could not be anymore tired and frustrated!!!!” she wrote to her regional center coordinator. “Is the only way Noah is going to get help [is] if I abandoned him and surrender him to the State!?!?”

Christine LyBurtus said she’s struggled to find the right care for Noah.
(Allen J. Schaben / Los Angeles Times)
::
Across the country, surging numbers of young people have landed in emergency rooms in the throes of a mental health crisis amid a shortage of needed care. Children in need of psychiatric care are routinely held in emergency departments for hours or even days. Even amid COVID, as people tried to avoid emergency rooms, mental health-related visits continued to rise among teens in 2021 and 2022.
Among those hit hardest by the crisis are autistic youth, who turn up in emergency rooms at higher rates than other kids — and are much more likely to do so for psychiatric issues. Many have overlapping conditions such as anxiety, and researchers have also found they face a higher risk of abuse and trauma.
“We’re a misunderstood, marginalized population of people” at higher risk of suicide, Lisa Morgan, founder of the Autism and Suicide Prevention Workgroup, said at a national meeting.
Yet the available assistance is “not designed for us.”
According to the National Autism Indicators Report, more than half of parents of autistic youth who were surveyed had trouble getting the mental health services their autistic kids needed, with 22% saying it was “very difficult” or “impossible.” A report commissioned by L.A. County found autistic youth were especially likely to languish in ERs amid few options for ongoing psychiatric treatment.

Karissa interacts with her brother, Noah, as he watches a video after school.
(Allen J. Schaben / Los Angeles Times)
In decades past, many psychiatrists were unwilling to diagnose mental health disorders in autistic people, believing “it was either part of the autism or for other reasons it was undiagnosable,” said Jessica Rast, an assistant research professor affiliated with the A.J. Drexel Autism Institute. Much more is now known about both autism and mental health treatment, but experts say the two fields aren’t consistently linked in practice.
Mental health providers may focus on an autism diagnosis for a prospective patient and say, “‘Well, that’s not in our wheelhouse. We’re treating things like depression or anxiety,’” said Brenna Maddox, assistant professor of psychiatry at the University of North Carolina School of Medicine.
Yet patients or their families “weren’t asking for autism treatment. They were asking for depression or anxiety or other mental health treatment,” Maddox said.
In the meantime, the system that serves children with developmental disabilities has faltered.
“Never have I seen that we can’t staff the needed things on so many cases,” Larry Landauer, executive director of the Regional Center of Orange County, said last year. Statewide, “there’s thousands and thousands of cases that are struggling.”
“If I’m a respite worker and I get called on to provide help to families … who am I going to select?” Landauer asked. “The [person] that watches TV and plays on his iPad and I just sit and monitor him? Or do I take someone that is significantly behaviorally challenged — that pulls my hair, that scares me all the time, that tries to run out the door? … Those are the ones getting left out.”
::
The fall and winter of 2022 were so trying that LyBurtus eventually took matters into her own hands. Noah bit his mother and smashed a bathroom window and tried to climb out before the Fullerton Fire Department arrived. Weeks later, LyBurtus had to dial 911 again after he bit his sister’s finger badly enough to draw blood.

Caregiver Terrence Morris, left, keeps a watchful eye on Noah.
(Mel Melcon / Los Angeles Times)
He ended up in a hold at Children’s Hospital of Orange County, which searched for another facility that might help him, but “all placement options declined patient placement,” according to his medical records.
Noah was again sent home with his mother, but the next day, he was back at Children’s Hospital of Orange County after slamming his head against a tile floor.
LyBurtus, frantic and bruised, made call after call and finally used her credit card to pay for an ambulance to take him to UCLA Resnick Neuropsychiatric Hospital, where he was admitted.
Week by week, psychiatrists there said Noah seemed to be making some strides as they adjusted his alphabet soup of medications. But hospital staff struggled to understand what would set him off.
Once, while playing cards, Noah suddenly started knocking the cards off the table and struck another patient in the face. Another day, he appeared suddenly to be frightened after using the bathroom, and then charged at a computer plugged in nearby.
But there were also days when he danced to a Michael Jackson song, or played Giant Jenga outside on the deck. One day, a doctor wrote, “He made eye contact for a few seconds. I waved to him, and he looked at his hand, as though he was wondering what to do with it in return.”

Christine LyBurtus washes her son’s face. When Noah was 3, a doctor noted he was a “very cute little boy” who played alone, rocked back and forth, and sometimes bit himself.
(Mel Melcon / Los Angeles Times)
LyBurtus was straining to find more help at home so UCLA held off on discharging him, but at the end of January 2023 Noah was sent home. With no changes in medication planned, “and the strong possibility that Noah grew tired of the inpatient setting, the ward no longer was deemed therapeutic or necessary,” a doctor wrote.
Less than a month later, he was back in the emergency room at Children’s Hospital of Orange County after biting and attacking his mother.
A psychiatrist at the pediatric hospital wrote that because he had limited ability to communicate, another round of psychiatric hospitalization would do little unless it was specialized for “individuals with neurodevelopmental needs.” When the 72-hour hold at children’s hospital ran out, LyBurtus asked for an ambulance to take Noah home, fearful of driving him herself.
In May, the month Noah turned 14, LyBurtus heard the regional center had found a place for Noah: a four-bed facility in Rio Linda, a tiny town near Sacramento that she’d never heard of. He could live there for more than a year, she was told, and then hopefully return home with the right support.

Christine LyBurtus shows photographs to Noah.
(Mel Melcon / Los Angeles Times)
But LyBurtus fretted about what she would do if something happened to him so far away. She felt, she said, like she had failed her child. Months passed as they waited for a spot there; LyBurtus said she was told they were trying to hire the needed staff.
“I don’t want him to go,” she said, “but I don’t want to continue going on the way that we’re going on.”
Then in August, LyBurtus was told the regional center had found a spot at a facility much closer to home: the state-run South STAR facility in Costa Mesa, about 20 miles from their apartment. Noah would occupy one of only 15 STAR beds across the state for developmentally disabled adolescents in “acute crisis.”
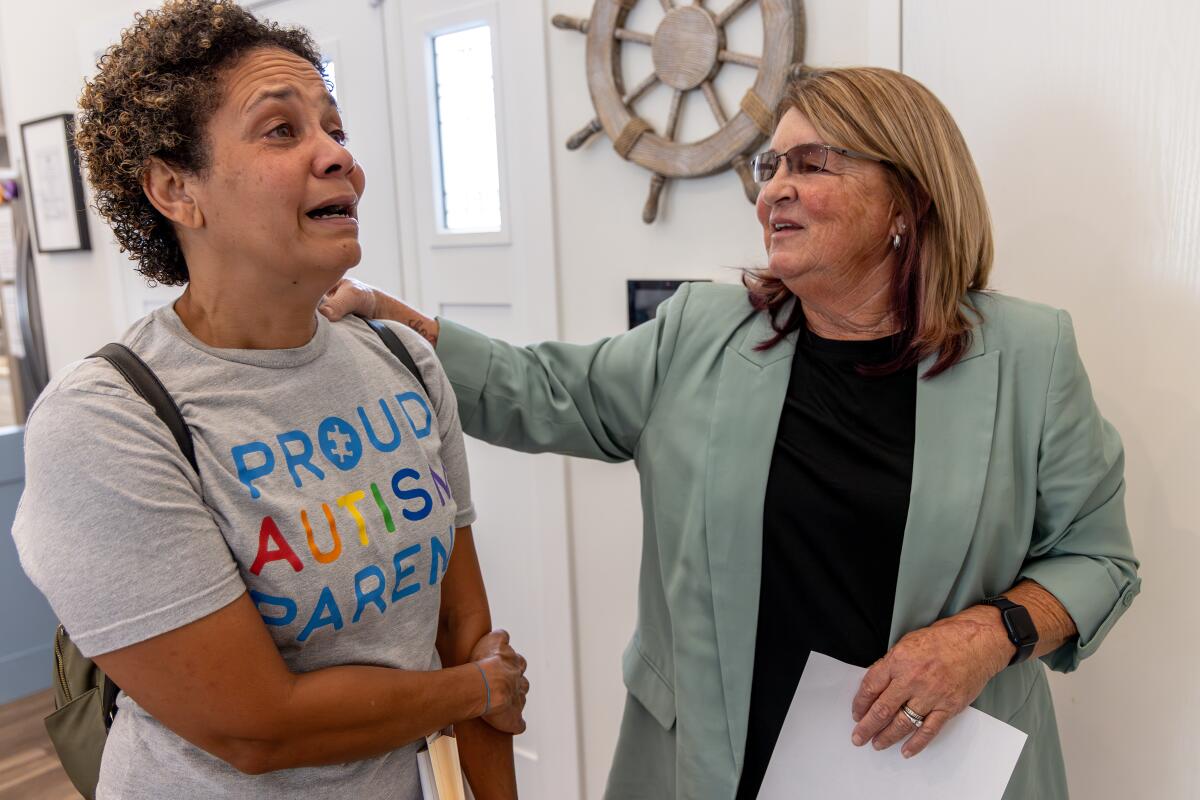
On a bright September morning, LyBurtus pulled up at an unassuming gray house with a “Home Sweet Home” sign by the door. The three teens living there were gone for the morning while an administrator and South STAR program director Kim Hamilton-Royse showed LyBurtus around the house.
Minutes into the tour, LyBurtus found herself crying. Hamilton-Royse stopped her explanation of the daily schedule. “I know this is super hard for you,” she said gently.
But LyBurtus brightened at the sight of the sensory room outfitted with crash pads and a mesmerizing, colorful cylinder of bubbling water. Hamilton-Royse pointed out a vibrating chair and added that they had a projector that would fill the room with illuminated stars.
LyBurtus took photos on her smartphone to show Noah. “You’re not going to be able to get him out of here,” she said.
As they rounded the rest of the house — bedrooms with dressers secured to the wall, a living room with paintings of sailboats, a fish tank — Hamilton-Royse asked if LyBurtus felt any better.

Christine LyBurtus reacts while boxing up items for Noah’s move.
(Mel Melcon / Los Angeles Times)
“I do,” she said. “I just hope that he can behave.”
Hamilton-Royse reassured her that South STAR had never kicked anyone out. “And we’ve had some really challenging folks,” she said.
“I promise you we’ll take very good care of him.”
As she returned to her car, LyBurtus took a deep breath. “It’s hard not to feel like I’m betraying him,” she said, her voice shaking. “But I can’t keep living like this, you know?”
1
2

3

1. Christine Lyburtus tours a residential care facility in Costa Mesa, about 20 minutes from her home. (Irfan Khan / Los Angeles Times) 2. At the South STAR facility, LyBurtus was told, Noah would occupy one of only 15 STAR beds across the state for developmentally disabled adolescents in “acute crisis.” (Irfan Khan / Los Angeles Times) 3. “I just hope that he can behave,” LyBurtus said of son Noah. (Irfan Khan / Los Angeles Times)
Three days later, Noah went back to the Children’s Hospital of Orange County on another psychiatric hold. He came home, then was back in the emergency department a week and a half later.
::
The October night before Noah left home, LyBurtus had brought home sushi for him, one of his favorite foods. He fell asleep around 6:30 p.m, and woke up again at 1 a.m. LyBurtus gave him his medication and as he drifted back to sleep, his mother held him, enjoying the peace.
When he woke up in the morning, she could tell he knew something was up. His clothes had been packed. She’d already shown him photos of the Costa Mesa home and told him, “This is where you’re going. I’m still your mom. I’m still going to go and see you.”

Noah embraces his mother shortly before he was picked up and driven to a residential care facility in Costa Mesa.
(Mel Melcon / Los Angeles Times)
When the black SUV arrived, LyBurtus offered Oreos to coax him into the unfamiliar car. She followed the SUV in her car, staying far enough behind to avoid having Noah see her when he arrived. LyBurtus had been told it would ease the transition.
Back at home, she sank into the bathtub, utterly spent. “I’m going to have to just go with trusting this process as much as I can,” she said, “because I don’t have another choice right now.”
The next day, she met with the South STAR staff to tell them more about Noah. What he likes to eat. What triggers him. His favorite things to do. The Costa Mesa home called whenever staff had physically restrained Noah, but when a weekend passed without a call, she felt some relief.
Lyburtus smiled at the photos and videos sent home: putting together an elaborate stacking toy, washing dishes. It felt like things were going well, LyBurtus said. The staff had scaled back the amount of psychiatric medication he was taking.
But more than a month later, when she first went to visit Noah, he excitedly took her to the front door, as if to say, “Let’s go,” she recalled. She gently told him she was just visiting.

Christine LyBurtus is comforted by caregivers Schahara Zad, left, and Terrence Morris after Noah moved into his residential care facility.
(Mel Melcon / Los Angeles Times)
He led her to the side door instead. She steered him away again. They stepped into the courtyard, and Noah immediately went to the gate to exit.
LyBurtus fell into a funk. As she worried about Noah, she was also figuring out how to make ends meet. With Noah in the Costa Mesa home, Lyburtus was no longer being paid more than $4,000 a month as his caregiver, her sole source of income for years. She tried a number of jobs but ultimately found the work that suited her: caregiving for an elderly woman and children with disabilities.
Her second and third visits with Noah were easier. She snapped photos — Mother and son nestled together on the couch. Noah touching her forehead.
The STAR program runs up to 13 months. As time passed, the regional center had started talking to her about where Noah would go next. LyBurtus was startled.
Wasn’t the plan for him to come home, she asked?

Christine LyBurtus, left, is briefed by Kim Hamilton-Royse while touring a residential care facility for her son.
(Irfan Khan/Los Angeles Times)
That was still on the table, LyBurtus said she was told. But if he wasn’t ready, they didn’t want to wait until the last minute to find somewhere else for Noah, who turned 15 in May.
LyBurtus wanted to block out the idea of him going to another facility.
“I never want to live the way we were living again,” she said.
“But is that worse than him being hours away? I don’t know.”

new video loaded: NASA Announces Artemis III Crew
transcript
transcript
NASA Announces Artemis III Crew
NASA announced the crew of Artemis III mission, which will fly to low-Earth orbit to test rendezvous and docking maneuvers with one or two lunar landers.
-
“I am excited to welcome you as the next crew in the Artemis journey to successfully return to the moon — this time to stay.” “I’m honored by the role that I’ve been given. I’m also very humbled by the task in front of us. But first and foremost, I’m grateful.” “So with that, the Artemis II crew, comrade, hands you the baton. You got the controls.” “As you know, we had a significant anomaly at our Launch Complex 36A on May 28. We’ve redoubled our efforts and are moving forward.”
By Alisa Shodiyev Kaff
June 9, 2026
Science
Santa Monica Mountains’ last steelhead trout survived the Palisades fire — and even had babies

Scientists feared the Santa Monica Mountains’ last remaining steelhead trout were dead, smothered by debris flows unleashed by the Palisades fire.
But the endangered fish surprised them: A team of biologists recently spotted 30 of the rare trout — and 21 babies — in Topanga Creek.
“There was a lot of happy dancing in the creek,” said Rosi Dagit, principal conservation biologist for the Resource Conservation District of the Santa Monica Mountains, which works with public and private landowners to conserve natural resources.
That’s because the steelhead here are endangered, at both the state and federal levels. Once, they swam in most streams of the Santa Monicas, but their numbers plummeted amid overfishing and coastal development. Increasingly frequent wildfire has further stressed their habitat. Topanga Creek, a biodiversity hot spot, is home to their last known population in the mountains that stretch from the Hollywood Hills to Point Mugu in Ventura County.
The trout that were spotted, including this one, are part of a distinct Southern California population that’s listed as endangered at the state and federal levels.
(RCDSMM Stream Team)
The California Department of Fish and Wildlife spearheaded a complex mission to rescue trout threatened by the Palisades fire that sparked in January 2025.
Time was of the essence. The fire hadn’t yet been fully contained. But rain was on the way, which would sweep massive amounts of sediment from the denuded hillsides into the water. Fish are often killed this way.
Crews stunned the fish with electricity, scooped them up in buckets, trucked them to a hatchery and ultimately moved them to Arroyo Hondo Creek in Santa Barbara County.
Within days, Topanga Creek was choked with mud. Some assumed the fish left behind were goners.
But in March, the conservation district’s team found four. The following month, when water conditions were clearer, they saw more.
“These fish continue to amaze me,” said Kyle Evans, environmental program manager for the state Department of Fish and Wildlife, who had seen the damage to the creek. “I had seen populations get wiped out in similar situations. So when I heard, I was thrilled.”
Evans surmises the fish that survived were in an area of the creek where less charred material and sediment were swept in.
“These fish likely hunkered down, were hiding under some rocks or places to try to get away from the main concentration of flow,” he said. “And luckily they weren’t buried.”
The ones that were spotted were fairly small, around 6 to 14 inches. Rainbow trout and steelhead trout are the same species, but with different lifestyles. If the fish remain in freshwater, they’ll be considered rainbows. However, they can migrate to the ocean and become steelhead, where they typically grow larger before returning to their natal waters to spawn.
Topanga Creek hasn’t fully recovered from the damage it sustained, but scientists say it’s looking better. Surveys last year were “so depressing,” Dagit said, with very few animals, and stretches that were essentially transformed into flat roads from all the sediment buildup. Some of the riparian canopy burned right down to the creek.
Then came 32 inches of rain over the last nine months, scouring out and moving sediment, creating deeper pools. Dagit said they recently found newt egg masses for the first time in years, as well as a few adult newts and many frogs. Plants that provide cover are starting to recover.
She provided photos comparing certain pools last year and this year, some dramatically transformed. In September 2025, the Shrine Pool could have been an overgrown hiking trail. This April, it was filled with shallow water.

The Shrine Pool in September 2025, left, and the same location in April 2026, right, with RCDSMM’s Isaac Yelchin donning a wetsuit.
(RCDSMM Stream Team)
Topanga Creek is home to another endangered fish, the small but hardy northern tidewater goby, often described as cute. Not long before the trout operation, Dagit led a rescue of hundreds of these fish too. Many were repatriated to the lagoon at the mouth of the creek in a moving ceremony last June.
There’s still the matter of what to do with the trout that were moved to Santa Barbara County last year. Evans would like to bring them home to the Santa Monicas at some point, but isn’t sure if it will happen. On one hand, they could bolster the small, genetically isolated surviving population. On the other, they might inadvertently bring in a disease or bacteria. There is some time to decide. Evans estimates the creek still needs to recover for two to three more years.
For now, the fish are functioning fine in their adopted creek. Experts worried the trauma wrought by the move would disrupt their spawning process, but they had babies that spring. This year, they spawned again.

The Pacifica Municipal Pier was shut down and taped off Thursday after city workers noticed cracks running through the landmark structure and concrete chunks falling into the ocean.
It’s just one of many coastal California structures that have recently crumbled under pressure from a rising and relentless ocean.
Officials from the small, beach city south of San Francisco said the pier was closed due to “cracking, separation, and displacement of the concrete walkway and structural elements.”
It will stay closed while structural engineers asses its safety.
Photos taken by city employees show a wide crack that runs from top to bottom and across the structure as well. Other photos show a large horizontal crack under the foundation of a small restaurant on the pier, the Chit Chat Cafe.
The cafe was also shut down.
This is not the first time the 53-year-old pier has shown signs of stress. In 2021, part of it was shut down after handrails along the edge collapsed. And in 2023, after a series of storms pummeled the Central California coast, damaging parts of the pier, the structure was partially closed for more than year.
Those same storms caused extensive damage in Aptos and Capitola, 70 miles south, where piers and waterfront infrastructure were swept away or damaged.
In 2024, a 150- to 180- foot section of the Santa Cruz wharf was ripped off by powerful waves.
At least 10 of the state’s dozens of coastal public piers were closed for part or all of 2024 due to structural damage sustained in winter storms since 2022. At least five others have longer-term upgrades planned to address structural issues.
“These things are costly to maintain,” said Zach Plopper, senior environmental director at Surfrider. “They are a part of our California coastal culture in many ways, but we’re going to need to reckon with, one, the state that they’re in, and two, the continuous and worsening threats they’re going to experience,”
He said most of the piers were constructed in the early 1900s, and they weren’t built to withstand decades of rough seas, storms and rising sea level.
“With this incoming El Niño, which is forecasted to be significant, and this marine heat wave we’re in the midst of, we’re kind of in uncharted waters as far as what this winter could bring in terms of storms and swells to the California coast, and we’re likely going to see a lot more damage,” he said. “Not just piers, but roads and other coastal infrastructure up and down the state.”
There was no storm in Pacifica earlier this week, so no single event could be blamed for the destruction.
However, a 2025 report from an outside engineering firm, GHD, found that several sections of the pier were in “poor” or “serious” condition, and they recommended closure before anticipated storms or events that could “subject the piles to high winds, swells and large waves.”
The firm found several areas of the pier where concrete was missing and rebar was exposed and corroding.
“The pier has continued to experience high winds and large waves in a harsh marine environment,” the engineers wrote in the report, noting that continuous exposure to seawater or marine spray was “detrimental” to the structure.
A 2023 city report estimated it would cost $19 million to repair.
That same year, a state law was enacted to require local governments along the California coast to plan for sea level rise in the coming decades.
Sea level has risen some 8 inches, on average, along the coast in the past 150 years, Plopper said, and researchers anticipate another foot in the next 25 years.
“We’re going to see profound shifts on our coastline, none that we have ever experienced before, and building static structures on the coast just doesn’t work all that well,” he said. “We’re going to have to make some really hard decisions.”
-

 Kentucky4 minutes ago
Kentucky4 minutes agoWhat states spend the most on fast food? Kentucky ranks among the top
-

 Louisiana11 minutes ago
Louisiana11 minutes agoWinnsboro woman dies in single-vehicle crash on LA Highway 867
-

 Maine13 minutes ago
Maine13 minutes agoLive updates: Midterms take shape in California, Maine, S.C. and Nevada; Trump to sign ICE bill
-

 Maryland19 minutes ago
Maryland19 minutes agoAlert Days Wednesday through Friday for severe weather risk, intense heat in Maryland
-

 Michigan26 minutes ago
Michigan26 minutes agoTrieu: For Michigan State targets, visits, in-state decisions loom
-

 Massachusetts28 minutes ago
Massachusetts28 minutes agoMake Father’s Day memorable with these 10 activities in Massachusetts
-

 Minnesota34 minutes ago
Minnesota34 minutes agoStrong winds, downed trees hit Twin Cities, cutting power to 50,000 in Minnesota
-

 Missouri38 minutes ago
Missouri38 minutes agoNew West Boulevard Elementary School principal announced

