Science
COVID and bird flu are rising. Here's how to keep yourself safe

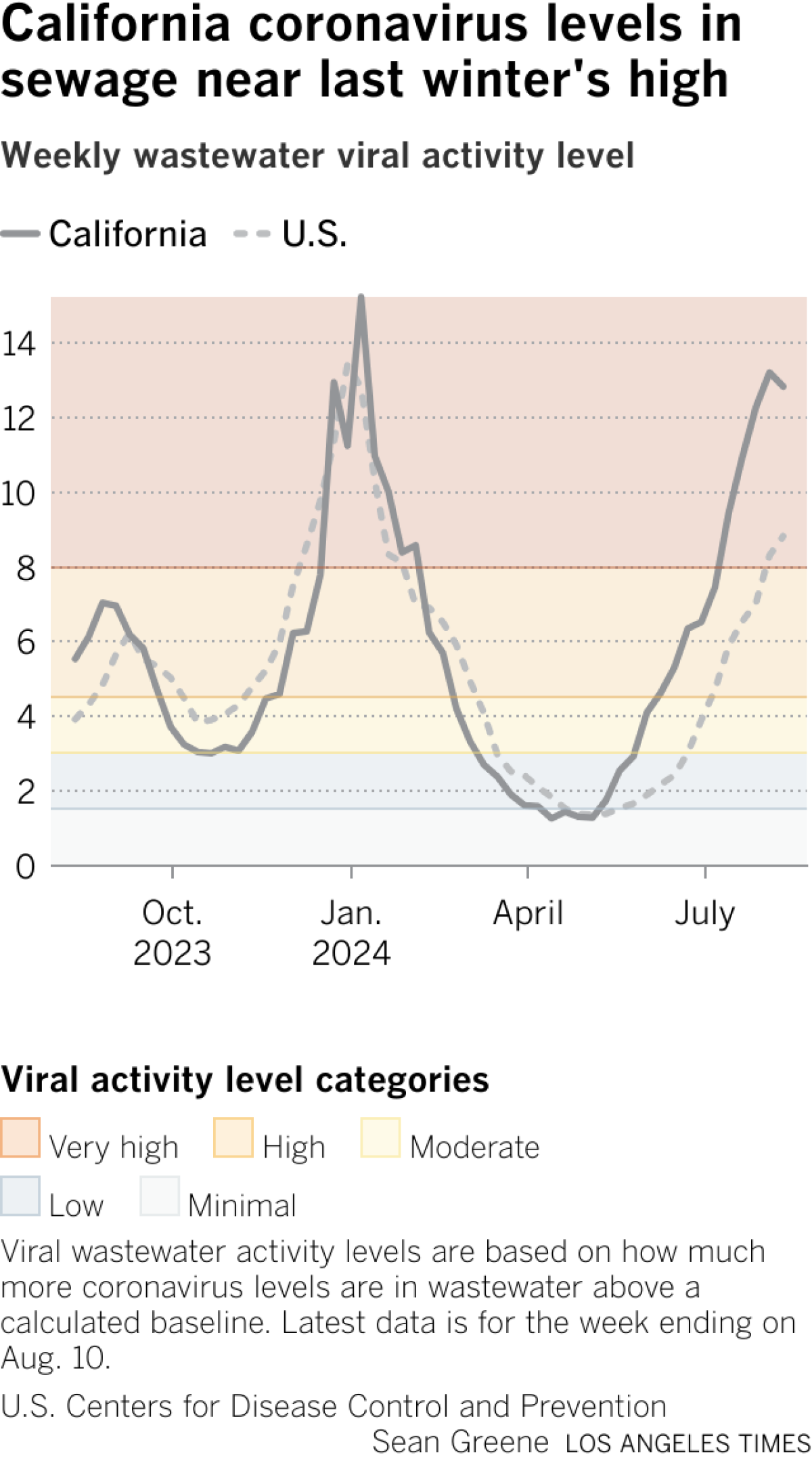
With California’s COVID surge at very high levels, doctors are urging people who are experiencing respiratory symptoms to test themselves or see a medical professional who can check on their illness.
This is the worst COVID summer infection spike in California since 2022, according to wastewater data. There are a number of possible culprits for the surge. A series of punishing heat waves and smoke from devastating wildfires have kept many Californians indoors, where the disease can more easily spread. Most adults are also well removed from their last brush with the coronavirus, or their last vaccine dose — meaning they’re more vulnerable to infection.
But changes in the virus have also widened the scope of the surge.
Of particular concern is the rise of a hyperinfectious subvariant known as KP.3.1.1, which is so contagious that even people who have eluded infection throughout the pandemic are getting sick.
“This is a very large surge that we are seeing currently. This is starting to rival, really, what we saw this past winter,” said Dr. Elizabeth Hudson, regional chief of infectious diseases at Kaiser Permanente Southern California.
Coronavirus levels in Los Angeles County wastewater are continuing to rise, according to the most recently available data. And viral levels in California wastewater are at “very high” levels as defined by the U.S. Centers for Disease Control and Prevention.
Coronavirus levels in the state’s wastewater were down 3% when comparing the week that ended Aug. 10 with the prior week, a possible indication that levels are cresting — although it’s also possible that coronavirus levels will increase again. Seasonal viral levels in sewage are expected to peak at some point, but it won’t be clear until a few weeks of consistent declines are observed.
Here are some things that experts say you can do to keep yourself safe:
Get tested
Doctors are urging people dealing with respiratory illness symptoms — including healthcare providers — to seek testing.
Dr. Abraar Karan, an infectious diseases expert and epidemiologist at Stanford University, said confirmation of a COVID-19 diagnosis would help a patient get a Paxlovid prescription to help treat the illness, while confirmation of another illness, like the flu, could help a patient get a drug more targeted toward that ailment.
An initial negative test does not mean you don’t have COVID; doctors suggest testing for as long as five days after the onset of symptoms to determine whether a test turns positive.
More consistent testing at medical facilities also could help detection of unusual strains that epidemiologists want to track, such as bird flu.
Bird flu has attracted attention recently because of outbreaks in poultry and dairy cows, and there have been several recent human cases among dairy and poultry workers in the U.S., according to the CDC.
The rise of bird flu
Recent human cases of H5N1 bird flu have resulted in primarily mild symptoms, including conjunctivitis, also known as pink eye, Karan said.
But one reason doctors are closely monitoring the situation is that, in the decades in which we’ve been aware of bird flu infecting humans, some H5N1 strains have resulted in significant mortality rates.
According to the CDC, human infections with H5N1 virus, which have been reported in 23 countries since 1997, have resulted in severe pneumonia and death in about 50% of cases.
Now that we know bird flu has infected cows, and there’s cow-to-human transmission, that poses a potential problem.
“Cow udders have receptors in common with birds, and they also have receptors in common with humans, where these viruses bind,” Karan said.
“Now, with human flu season coming, you have the risk of what’s called viral reassortment, where a host can get infected with both bird flu and human flu at the same time, and those flus now start swapping genetic material,” Karan said. “This is kind of how swine flu happened [in 2009]. So this is where we’re really worried. It’s like a ticking time bomb of human flu season around the corner, and yet we still have this uncontrolled spread of bird flu in cows.”
Bird flu hasn’t resulted in sustained human-to-human transmission, nor caused a pandemic in humans, in recent times.
“But it’s one of those pathogens that’s high risk of mutating to a point of increasing transmissibility. And the pathogen has had high virulence based on historical cases. … It’s the risk of where it could go,” Karan said.
Tracking the spread
This illustrates why it can be important for patients to get tested. If a test shows that a person has the flu, subsequent screening — including genetic subtyping — could eventually determine whether it is bird flu. And that could help epidemiologists figure out how the bird flu may have spread and help doctors determine the best course of treatment.
Even if a case of bird flu results in mild symptoms, it’s important to diagnose it, Karan said, so the virus sample can be genetically analyzed and scientists can track where it jumped from animal to human, and potentially more aggressively treat the patient with antivirals.
“But imagine — that only happens if I even test that patient for flu at all,” Karan said.
Where bird flu stands in the U.S.
Since 2022, according to the CDC, there have been 14 reported human cases of H5 bird flu in the U.S., 13 of which have been reported since March 24. Of the 14, nine have been confirmed as H5N1.
Of the 14 cases of bird flu in humans, 10 followed exposure to poultry, and the remainder followed exposure to cows. All of the reported human cases have occurred in three states: Colorado, Michigan and Texas.
Nationally, there are 48 states with bird flu outbreaks in poultry and 13 with outbreaks in dairy cows.
Since 2022, more than 100 million birds in the U.S. have been reported to have been infected with bird flu, including commercial poultry, backyard or hobbyist flocks and wild aquatic birds; it’s the first detection of this type of flu virus in the U.S. since 2016.
Bird flu has been detected in wild birds in most counties of California, including all of Southern California and the San Francisco Bay Area, and most of the Central Valley.
Bird flu outbreaks — those involving commercial poultry facilities or backyard poultry and hobbyist bird flocks — in California have been reported in just one county in Southern California: San Diego County. Bird flu outbreaks have occurred in a number of counties in Northern and Central California, including Sacramento, Contra Costa, Fresno, San Francisco, San Joaquin, Stanislaus, Sonoma, Monterey, Placer, Merced and Marin counties.
As for bird flu infecting dairy cows, 13 states have reported outbreaks — Idaho, Wyoming, Colorado, New Mexico, Texas, Oklahoma, Kansas, South Dakota, Minnesota, Iowa, Michigan, Ohio and North Carolina. In the last month, outbreaks infecting dairy cows have affected five states: Idaho, Colorado, Texas, South Dakota and Michigan.
In May, there was a detection of bird flu in a live bird market in San Francisco, according to the California Department of Food and Agriculture. State officials urged people to separate poultry from wild birds if possible.
“Because of the recent case in California poultry production and epidemiologic evidence that this strain was introduced by wild birds, we ask that California producers move their birds indoors through December 2024,” the California Department of Food and Agriculture said in June.
Protecting family and friends
The CDC earlier this year eased COVID isolation guidance, given that the health impacts of COVID-19 are lower than they once were, thanks to the availability of vaccines, anti-COVID medicines and increased population immunity.
There are fewer people being hospitalized and dying, and fewer reports of complications such as multi-inflammatory syndrome in children.
Still, doctors say it remains prudent to take common-sense steps to avoid illness and spreading the disease to others, given that COVID still causes significant health burdens that remain worse than the flu. Nationally, since the start of October, more than 49,000 people have been reported to have died of COVID; by contrast, flu has resulted in at least 25,000 fatalities over the same time period, according to federal estimates, which will be updated later this year.
While the prevalence of long COVID has been going down, long COVID can still be a risk any time someone gets COVID.
Doctors are urging everyone to get up to date on vaccinations — particularly if patients are at higher risk of severe complications from COVID-19. An updated COVID-19 vaccination formula is expected to become available in a matter of week, and the CDC is urging everyone 6 months and older to get one dose of the updated vaccine.
In California, just 37% of seniors 65 and older have received the last updated COVID-19 vaccine that first became available in September.
It’s especially important that older people get at least one updated dose. Of the patients he has seen recently who had serious COVID, UC San Francisco infectious diseases specialist Dr. Peter Chin-Hong said none of them had gotten an updated vaccine in the last year.
Avoid sick people. Some who are infected might pass off their symptoms simply as a cold or allergies when it could be the start of a COVID-19 illness.
Test if you’re sick, and test repeatedly if your first test shows up as negative.
An initial negative test doesn’t mean you don’t have COVID; doctors suggest testing for as long as five days after the onset of symptoms to check whether a test turns positive.
Consider taking a rapid COVID test once a day for three to five consecutive days after the onset of cough-and-cold symptoms, Hudson said.
Doing so can help a person take measures to later isolate themselves and limit spread of the illness to others.
Masks are much less common these days but can still be a handy tool to prevent infection. Wearing a mask on a crowded flight or in a crowded indoor venue where people nearby are coughing can help reduce the risk of infection.
The best mask is one that is well-fitted and that you find comfortable wearing. The most protective are N95 respirators, followed by KN95 respirators and KF94s. Surgical masks offer more protection than cloth masks.
Have a plan to ask for Paxlovid if you become ill. Paxlovid is an antiviral drug that, when taken by people at risk for severe COVID-19 who have mild-to-moderate illness, reduces the risk of hospitalization and death.
And if you get Paxlovid, make sure to take the full five-day course of treatment. Don’t stop taking the drug halfway through the dose.
There are also other anti-COVID medications that are available, such as remdesivir, which is given intravenously, and molnupiravir, which is given orally, like Paxlovid.
- Stay away from others while sick
The CDC recommends people stay home and away from others until at least 24 hours after their respiratory viral symptoms are getting better overall and they have not had a fever without using fever-reducing medicine such as Tylenol or Advil. Previously, the CDC suggested people with COVID isolate for at least five days and take additional precautions for a few more days.
In terms of deciding when symptoms are getting better, what’s most important is “the overall sense of feeling better and the ability to resume activities,” the CDC says. A lingering cough by itself can last beyond when someone is contagious, the CDC said.
But the CDC also advises added precautions for five additional days to avoid infecting others, such as wearing a mask, opening windows to improve air circulation, washing hands often, keeping one’s distance from others and continuing to test. It’s possible for infected people to be contagious even after they feel better.
The Los Angeles County Department of Public Health suggests infected people who have symptoms get a negative test result before leaving isolation. The agency also suggests those who are infected — regardless of whether they have symptoms — wear a mask around others for 10 days after they start feeling sick or, if asymptomatic, their first positive test result. However, they can remove their mask sooner if they have two sequential negative tests at least one day apart.
The agency suggests staying away from the elderly and immunocompromised people for 10 days after you start to feel sick, or, if asymptomatic, after their first positive test result.
If patients recover and then get sick again, they may have COVID rebound and need to stay home and isolate from non-infected people in their household.

new video loaded: NASA Announces Artemis III Crew
transcript
transcript
NASA Announces Artemis III Crew
NASA announced the crew of Artemis III mission, which will fly to low-Earth orbit to test rendezvous and docking maneuvers with one or two lunar landers.
-
“I am excited to welcome you as the next crew in the Artemis journey to successfully return to the moon — this time to stay.” “I’m honored by the role that I’ve been given. I’m also very humbled by the task in front of us. But first and foremost, I’m grateful.” “So with that, the Artemis II crew, comrade, hands you the baton. You got the controls.” “As you know, we had a significant anomaly at our Launch Complex 36A on May 28. We’ve redoubled our efforts and are moving forward.”
By Alisa Shodiyev Kaff
June 9, 2026
Science
Santa Monica Mountains’ last steelhead trout survived the Palisades fire — and even had babies

Scientists feared the Santa Monica Mountains’ last remaining steelhead trout were dead, smothered by debris flows unleashed by the Palisades fire.
But the endangered fish surprised them: A team of biologists recently spotted 30 of the rare trout — and 21 babies — in Topanga Creek.
“There was a lot of happy dancing in the creek,” said Rosi Dagit, principal conservation biologist for the Resource Conservation District of the Santa Monica Mountains, which works with public and private landowners to conserve natural resources.
That’s because the steelhead here are endangered, at both the state and federal levels. Once, they swam in most streams of the Santa Monicas, but their numbers plummeted amid overfishing and coastal development. Increasingly frequent wildfire has further stressed their habitat. Topanga Creek, a biodiversity hot spot, is home to their last known population in the mountains that stretch from the Hollywood Hills to Point Mugu in Ventura County.
The trout that were spotted, including this one, are part of a distinct Southern California population that’s listed as endangered at the state and federal levels.
(RCDSMM Stream Team)
The California Department of Fish and Wildlife spearheaded a complex mission to rescue trout threatened by the Palisades fire that sparked in January 2025.
Time was of the essence. The fire hadn’t yet been fully contained. But rain was on the way, which would sweep massive amounts of sediment from the denuded hillsides into the water. Fish are often killed this way.
Crews stunned the fish with electricity, scooped them up in buckets, trucked them to a hatchery and ultimately moved them to Arroyo Hondo Creek in Santa Barbara County.
Within days, Topanga Creek was choked with mud. Some assumed the fish left behind were goners.
But in March, the conservation district’s team found four. The following month, when water conditions were clearer, they saw more.
“These fish continue to amaze me,” said Kyle Evans, environmental program manager for the state Department of Fish and Wildlife, who had seen the damage to the creek. “I had seen populations get wiped out in similar situations. So when I heard, I was thrilled.”
Evans surmises the fish that survived were in an area of the creek where less charred material and sediment were swept in.
“These fish likely hunkered down, were hiding under some rocks or places to try to get away from the main concentration of flow,” he said. “And luckily they weren’t buried.”
The ones that were spotted were fairly small, around 6 to 14 inches. Rainbow trout and steelhead trout are the same species, but with different lifestyles. If the fish remain in freshwater, they’ll be considered rainbows. However, they can migrate to the ocean and become steelhead, where they typically grow larger before returning to their natal waters to spawn.
Topanga Creek hasn’t fully recovered from the damage it sustained, but scientists say it’s looking better. Surveys last year were “so depressing,” Dagit said, with very few animals, and stretches that were essentially transformed into flat roads from all the sediment buildup. Some of the riparian canopy burned right down to the creek.
Then came 32 inches of rain over the last nine months, scouring out and moving sediment, creating deeper pools. Dagit said they recently found newt egg masses for the first time in years, as well as a few adult newts and many frogs. Plants that provide cover are starting to recover.
She provided photos comparing certain pools last year and this year, some dramatically transformed. In September 2025, the Shrine Pool could have been an overgrown hiking trail. This April, it was filled with shallow water.

The Shrine Pool in September 2025, left, and the same location in April 2026, right, with RCDSMM’s Isaac Yelchin donning a wetsuit.
(RCDSMM Stream Team)
Topanga Creek is home to another endangered fish, the small but hardy northern tidewater goby, often described as cute. Not long before the trout operation, Dagit led a rescue of hundreds of these fish too. Many were repatriated to the lagoon at the mouth of the creek in a moving ceremony last June.
There’s still the matter of what to do with the trout that were moved to Santa Barbara County last year. Evans would like to bring them home to the Santa Monicas at some point, but isn’t sure if it will happen. On one hand, they could bolster the small, genetically isolated surviving population. On the other, they might inadvertently bring in a disease or bacteria. There is some time to decide. Evans estimates the creek still needs to recover for two to three more years.
For now, the fish are functioning fine in their adopted creek. Experts worried the trauma wrought by the move would disrupt their spawning process, but they had babies that spring. This year, they spawned again.

The Pacifica Municipal Pier was shut down and taped off Thursday after city workers noticed cracks running through the landmark structure and concrete chunks falling into the ocean.
It’s just one of many coastal California structures that have recently crumbled under pressure from a rising and relentless ocean.
Officials from the small, beach city south of San Francisco said the pier was closed due to “cracking, separation, and displacement of the concrete walkway and structural elements.”
It will stay closed while structural engineers asses its safety.
Photos taken by city employees show a wide crack that runs from top to bottom and across the structure as well. Other photos show a large horizontal crack under the foundation of a small restaurant on the pier, the Chit Chat Cafe.
The cafe was also shut down.
This is not the first time the 53-year-old pier has shown signs of stress. In 2021, part of it was shut down after handrails along the edge collapsed. And in 2023, after a series of storms pummeled the Central California coast, damaging parts of the pier, the structure was partially closed for more than year.
Those same storms caused extensive damage in Aptos and Capitola, 70 miles south, where piers and waterfront infrastructure were swept away or damaged.
In 2024, a 150- to 180- foot section of the Santa Cruz wharf was ripped off by powerful waves.
At least 10 of the state’s dozens of coastal public piers were closed for part or all of 2024 due to structural damage sustained in winter storms since 2022. At least five others have longer-term upgrades planned to address structural issues.
“These things are costly to maintain,” said Zach Plopper, senior environmental director at Surfrider. “They are a part of our California coastal culture in many ways, but we’re going to need to reckon with, one, the state that they’re in, and two, the continuous and worsening threats they’re going to experience,”
He said most of the piers were constructed in the early 1900s, and they weren’t built to withstand decades of rough seas, storms and rising sea level.
“With this incoming El Niño, which is forecasted to be significant, and this marine heat wave we’re in the midst of, we’re kind of in uncharted waters as far as what this winter could bring in terms of storms and swells to the California coast, and we’re likely going to see a lot more damage,” he said. “Not just piers, but roads and other coastal infrastructure up and down the state.”
There was no storm in Pacifica earlier this week, so no single event could be blamed for the destruction.
However, a 2025 report from an outside engineering firm, GHD, found that several sections of the pier were in “poor” or “serious” condition, and they recommended closure before anticipated storms or events that could “subject the piles to high winds, swells and large waves.”
The firm found several areas of the pier where concrete was missing and rebar was exposed and corroding.
“The pier has continued to experience high winds and large waves in a harsh marine environment,” the engineers wrote in the report, noting that continuous exposure to seawater or marine spray was “detrimental” to the structure.
A 2023 city report estimated it would cost $19 million to repair.
That same year, a state law was enacted to require local governments along the California coast to plan for sea level rise in the coming decades.
Sea level has risen some 8 inches, on average, along the coast in the past 150 years, Plopper said, and researchers anticipate another foot in the next 25 years.
“We’re going to see profound shifts on our coastline, none that we have ever experienced before, and building static structures on the coast just doesn’t work all that well,” he said. “We’re going to have to make some really hard decisions.”
-

 Maryland4 minutes ago
Maryland4 minutes agoAlert Days Wednesday through Friday for severe weather risk, intense heat in Maryland
-

 Michigan11 minutes ago
Michigan11 minutes agoTrieu: For Michigan State targets, visits, in-state decisions loom
-

 Massachusetts13 minutes ago
Massachusetts13 minutes agoMake Father’s Day memorable with these 10 activities in Massachusetts
-

 Minnesota19 minutes ago
Minnesota19 minutes agoStrong winds, downed trees hit Twin Cities, cutting power to 50,000 in Minnesota
-

 Missouri23 minutes ago
Missouri23 minutes agoNew West Boulevard Elementary School principal announced
-

 Mississippi26 minutes ago
Mississippi26 minutes agoHow Britain Became as Poor as Mississippi
-

 Montana34 minutes ago
Montana34 minutes agoDEQ to host Big Hole River water quality open house in Divide
-

 Nebraska41 minutes ago
Nebraska41 minutes agoNebraska pitcher enters transfer portal

